Diffuse Large B-cell Lymphoma Arising in the Spleen
Roberto N. Miranda, MD
Key Facts
Terminology
Primary DLBCL of spleen is rare
Involvement of splenic hilar lymph nodes and bone marrow (usually focal) can occur in primary DLBCL
Liver involvement may be part of definition of primary DLBCL of spleen with micronodular or diffuse patterns
Patients with history of DLBCL or dissemination at diagnosis are excluded (secondary DLBCL)
Clinical Issues
Adults are mainly affected; median age: 64 years
80% 5-year survival for primary DLBCL presenting as distinct mass
Macroscopic Features
Solitary or multiple distinct nodular masses surrounded by nonneoplastic spleen
Microscopic Pathology
Sheets of large cells with variable cytomorphology
B-cell lineage and surface immunoglobulin light chain restriction
Top Differential Diagnoses
Diffuse large B-cell lymphoma, systemic
Peripheral T-cell lymphoma
T-cell/histiocyte-rich large B-cell lymphoma
Classical Hodgkin lymphoma
Diagnostic Checklist
Single or multiple masses composed of large B cells
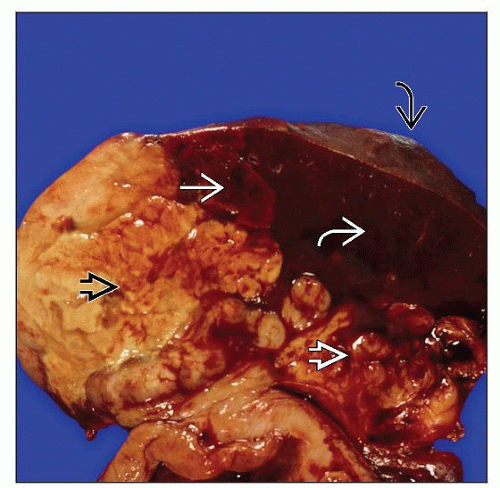 Gross photograph shows a multinodular tumor  . Tumor extends into hilar fat . Tumor extends into hilar fat  and shows focal infarction and shows focal infarction  . Well-preserved spleen is dark brown . Well-preserved spleen is dark brown  . Spleen capsule is noted . Spleen capsule is noted  . . |
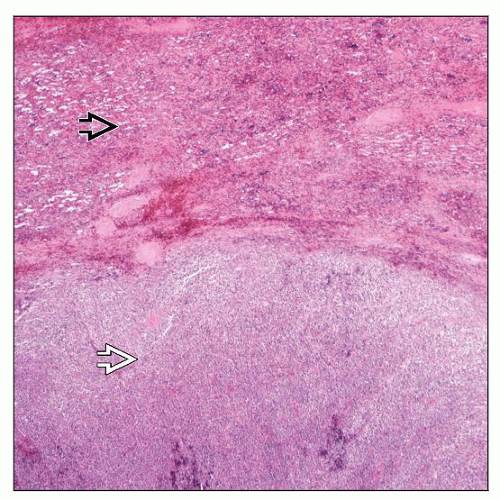 Hematoxylin and eosin shows the most common presentation of DLBCL characterized by a well-circumscribed tumor mass  surrounded by nonneoplastic spleen surrounded by nonneoplastic spleen  . . |
TERMINOLOGY
Abbreviations
Diffuse large B-cell lymphoma (DLBCL)
Synonyms
Large cell lymphoma
Definitions
Diffuse large B-cell lymphoma that arises in spleen
Involvement of splenic hilar lymph nodes and bone marrow (usually focal) can occur in primary DLBCL
Liver involvement may be part of definition of splenic DLBCL with micronodular or diffuse patterns
Primary DLBCL of spleen can be associated with splenic marginal zone B-cell lymphoma
Primary DLBCL of spleen is rare, but represents up to 40% of splenectomy specimens involved by DLBCL
Patients with history of lymphoma or evidence of disseminated DLBCL at diagnosis are excluded (secondary DLBCL)
ETIOLOGY/PATHOGENESIS
Infectious Agents
No known etiology
Primary DLBCL of spleen is rarely associated with hepatitis C or Epstein-Barr virus infection
CLINICAL ISSUES
Epidemiology
Age
Adults are mainly affected; median age: 64 years
M:F ratio approximately 1:1
Presentation
Abdominal pain
Pain is often left-sided
Systemic symptoms such as fever, malaise, and weight loss often occur
Fine needle aspiration may yield necrosis only and be wrongly diagnosed as splenic abscess
Diagnosis can be suspected in presence of splenomegaly and abdominal or retroperitoneal adenopathy
Most patients are immunocompetent
Occasionally reported in HIV(+) patients
Treatment
Chemotherapy similar to systemic cases of DLBCL
R-CHOP is most common chemotherapy used
Splenectomy usually performed for diagnostic purposes
Prognosis
80% 5-year survival for patients with primary DLBCL presenting as mass
Poor survival for DLBCL with T-cell-rich pattern or neoplasms that diffusely replace spleen
These cases often have disseminated disease shown by staging (probably not primary)
MACROSCOPIC FEATURES
General Features
Most cases show solitary or multiple distinct nodular masses surrounded by nonneoplastic spleen
Neoplasms that diffusely replace red pulp can be subtle grossly
Splenic weight can range from normal to > 3,000 g (average: 1,000 g)
Tumor size usually ranges from 5-18 cm
Multinodular tumor can replace up to 90% of spleen
Extensive necrosis is usual
Tumor may extend through capsule into adjacent diaphragm, stomach, pancreas, or abdominal wall
MICROSCOPIC PATHOLOGY
Histologic Features
Primary splenic DLBCL usually presents as large nodule or mass
Nodule/mass typically destroys white and red pulp
Approximately 1/3 of cases involve white pulp exclusively or predominantly
Approximately 20% of cases involve red pulp predominantly and diffusely
Adjacent Malpighian corpuscles may be focally involved
Variable cell morphology (centroblastic, immunoblastic, anaplastic, etc.)
Relative increased frequency of immunoblastic cases
Necrosis within neoplasm is common; sclerosis within or around neoplasm can be observed
Surrounding uninvolved spleen is distinctly separated from tumor, sometimes by fibrous bands
Predominant Pattern/Injury Type
Lymphoid, diffuse
Predominant Cell/Compartment Type
Hematopoietic, lymphoid
Immunophenotype
Neoplasms are of B-cell lineage: CD19(+), CD20(+), CD22(+), and pax-5(+)
Surface immunoglobulin light chain restriction is detected by flow cytometry in most cases
Most cases express Bcl-6 and about 1/3 express CD10
CD43 is positive in 20-30% of cases
CD3(−), CD5(−), CD23(−/+)
Absence of follicular dendritic cells (CD21, CD23) in tumor nodules
Cytogenetic and Molecular Findings
Monoclonal IgH rearrangements; TCR genes are usually germline
No distinctive cytogenetic or molecular findings
DIFFERENTIAL DIAGNOSIS
Diffuse Large B-cell Lymphoma (DLBCL), Systemic
Gross, microscopic, immunophenotypic, and molecular features can be identical to DLBCL arising in spleen
Distinction can be made after complete staging
Most DLBCL of spleen represent systemic or secondary involvement
T-cell/Histiocyte-rich Large B-cell Lymphoma (TCRLBCL)
Subtype of DLBCL that if identified in spleen, is suggestive of disseminated disease
Similar to any DLBCL both grossly and microscopically
Predominance of small T lymphocytes; large neoplastic B cells represent < 10% of cell infiltrate
Recently described micronodular variant (MTCRBL) does not produce large discrete mass but micronodules
MTCRBL distributed mainly in white pulp leaving no residual normal white pulp
DLBCL Primarily Involving Red Pulp
Unusual variant, clinically aggressive; median age: 69 years
Diffuse splenic involvement, predominantly in splenic cords
Frequent bone marrow and liver sinusoids infiltration; rare lymph node involvement
Mature B cells that usually coexpress CD5; Cyclin-D1 and CD23 negative
Peripheral T-cell Lymphoma (PTCL)
May involve white or red pulp
Cell composition is more polymorphic than DLBCL with mixture of eosinophils and plasma cells
Vascularity is often increased
Some cases may have increased histiocytes as well as erythrophagocytosis
Neoplastic cells including large cells react with T-cell markers (CD2, CD3, CD5, CD7); usually CD4(+)
Classical Hodgkin Lymphoma
Mainly involves white pulp
Scattered large Reed-Sternberg and Hodgkin cells in inflammatory background with eosinophils
Neoplastic cells are CD15(+), CD30(+), CD45(−), pax-5 (usually dim[+])
Nodular Lymphocyte-predominant Hodgkin Lymphoma (NLPHL)
Mainly involves white pulp
Predominance of small lymphocytes and scattered large cells with “popcorn” nuclei
Large neoplastic cells react with B-cell markers as well as with EMA and may be surrounded by small T cells
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


