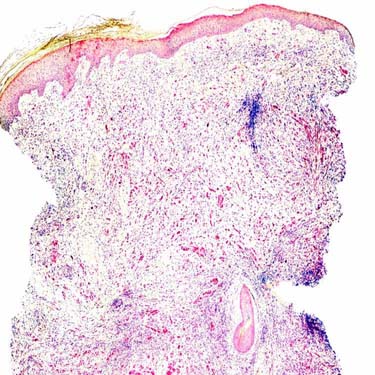
Scar-Like Appearance in DM Desmoplastic melanoma (DM) may resemble an inflamed scar on a low-power examination. However, aggregates of lymphoid cells and prominent solar elastosis are usually identified and are helpful findings.
Cytological Atypia in DM Unlike a scar, DM under high-magnification examination shows hyperchromatic-staining atypical spindle cells surrounded by abundant collagen bundles.
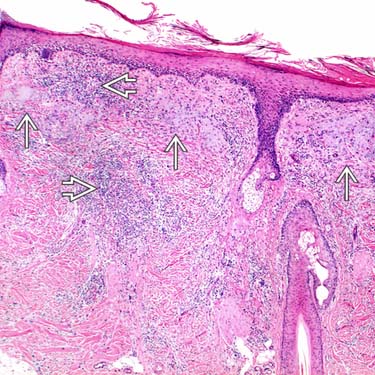
Dermal Lymphoid Aggregates in DM This punch biopsy shows hyperkeratosis overlying an expanded dermis, mimicking an inflamed scar. There are discrete lymphoid aggregates throughout the dermis that should raise suspicion for DM.
SOX10 Immunohistochemistry in DM The presence of scar-like dermis and multiple lymphoid aggregates should be followed up by SOX10 (or S100) immunohistochemistry to confirm DM as in this case. The nuclei of tumor cells are strongly positive.
TERMINOLOGY
Abbreviations
• Desmoplastic melanoma (DM)
Synonyms
• Desmoplastic/neurotropic melanoma
Definitions
• Form of invasive melanoma composed of spindle cells associated with dense stromal collagen
Resembles scar
CLINICAL ISSUES
Epidemiology
• Age
Presents in sun-damaged skin of elderly adults
Presentation
• Firm, skin-colored, tan or pink plaque or nodule
• Sometimes depressed
• Often amelanotic
Treatment
• Surgical approaches
It is important to resect DMs with clear surgical margins
– Needs to be done as early as possible for successful clinical management
There is increasing evidence that sentinel lymph node biopsy may not be indicated for “pure” variants
– This variant has low incidence of regional lymph node metastases
Prognosis
• Tumor thickness (Breslow depth)
• Clark level (IV vs. V)
• Histological subtype: Pure (longer disease-free survival) vs. combined
Pure subtype is defined as > 90% scar-like areas
Combined subtype is defined as densely cellular spindle cell collections
– Lacks significant scar-like areas (> 10%)
• Tumor mitotic rate
MICROSCOPIC
Histologic Features
• Ill-defined spindle cell neoplasm with highly infiltrative pattern of growth
• Overlying epidermis may show melanoma in situ (usually lentigo maligna type)
• Stromal collagen on scanning magnification resembles scar
• Spindle cells are arranged in fascicles and merge with scar-like areas
• Cellular density and cytologic atypia can vary based on histologic subtype
• Discrete dermal lymphoid aggregates
• Solar elastosis
Cytologic Features
• Pure subtype shows
Spindle cells with often deceptively mild cytological atypia
Nuclear hyperchromasia
Irregular nuclear contours
Minimal nuclear pleomorphism
Only gold members can continue reading. Log In or Register to continue



 and prominent solar elastosis
and prominent solar elastosis  are usually identified and are helpful findings.
are usually identified and are helpful findings.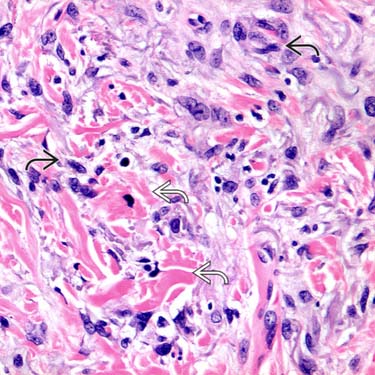
 surrounded by abundant collagen
surrounded by abundant collagen  bundles.
bundles.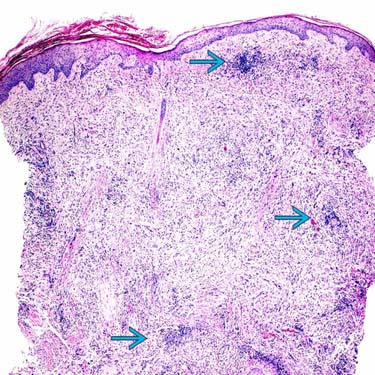
 throughout the dermis that should raise suspicion for DM.
throughout the dermis that should raise suspicion for DM.