Patient Story
A 55-year-old Hispanic woman presents to her family physician with a diffuse rash and increasing muscle weakness. The initial rash (without weakness) 2 months prior was thought to be a photosensitivity reaction to her new hydrochlorothiazide (HCTZ) prescription. She stopped the HCTZ and the rash initially improved with some topical corticosteroids. At the time of her current presentation, she had trouble getting up from a chair, walking, and lifting her arms over her head. The rash was prominent in sun-exposed areas, but was also seen in a shawl-like distribution in non-sun-exposed areas (Figure 181-1). Aside from her hypertension and obesity, the patient did not have any previous chronic medical conditions. She was afebrile with no other pertinent findings on physical exam.
Figure 181-1

Initial presentation of dermatomyositis in a 55-year-old Hispanic woman. Prominent violaceous erythema with scale is visible on the chest, face, and arms. Deep-red erythema is especially visible on the side of the face. The scalp is red and scaling. (Courtesy of Richard P. Usatine, MD.)
This is a classic presentation of dermatomyositis with the typical rash and proximal muscle weakness. Close attention to the rash around her eyes demonstrates the pathognomonic heliotrope rash of dermatomyositis (Figures 181-2 and 181-3). Also the patient has Gottron papules on the fingers, seen best in this case over the proximal interphalangeal (PIP) joint of the third finger (Figure 181-4). There was periungual erythema and ragged cuticles. The scalp was red and scaly. Her neurologic exam was consistent with proximal myopathy. She also had some trouble swallowing bread; and dysphagia is not unusual in dermatomyositis. Laboratory tests showed mild elevations in muscle enzymes with the aspartate aminotransferase (AST) having the greatest elevation. In other cases, the creatine kinase (CK) can be very elevated.
Figure 181-2
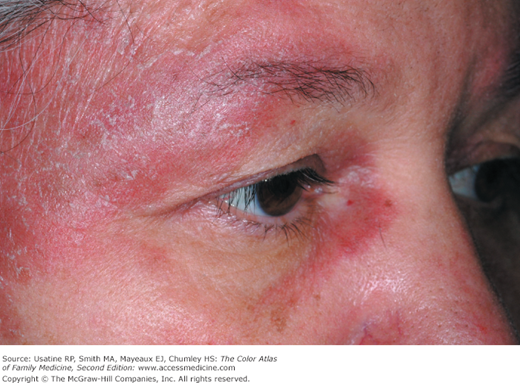
Close-up of the heliotrope (violaceous) rash around the eyes of the patient in Figure 181-1. (Courtesy of Richard P. Usatine, MD.)
Figure 181-3

View showing the bilateral heliotrope rash of the patient in Figure 181-1. A pathognomonic sign of dermatomyositis. (Courtesy of Richard P. Usatine, MD.)
Figure 181-4
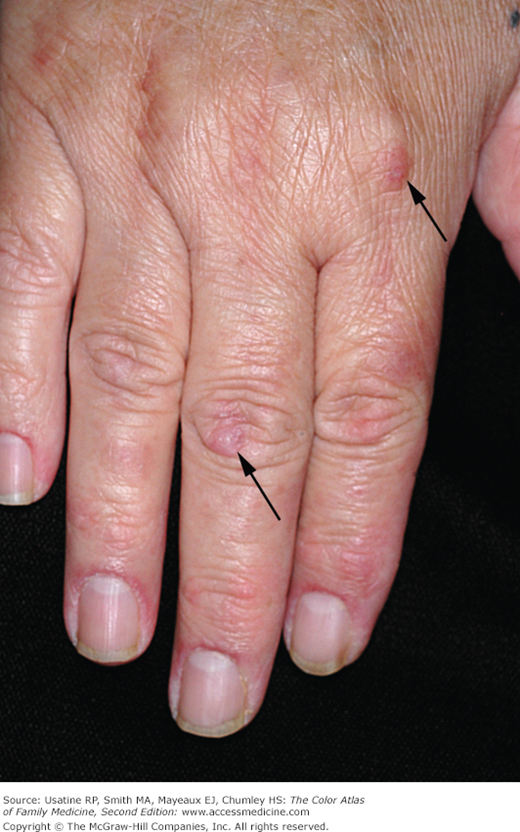
Hand involvement showing two Gottron papules over the knuckles (arrows) end erythematous nailfolds (periungual erythema) on the patient in Figure 181-1. (Courtesy of Richard P. Usatine, MD.)
The family physician started the patient on 60 mg of prednisone daily and topical steroids for the affected areas. The patient responded well to prednisone and 2 weeks later was feeling stronger and the rash was fading (Figure 181-5). After 4 weeks of 60 mg/day of prednisone she was started on 10 mg/wk of methotrexate in order to eventually taper her steroids. The patient has continued to do well, but the rash and muscle weakness tend to recur when her steroids are being tapered. The patient was sent for physical therapy and started on calcium and vitamin D supplementation to protect her from steroid-induced osteoporosis. She was also given 1 mg/day of folic acid to minimize the adverse effects of methotrexate. As dermatomyositis may be precipitated by an underlying malignancy, the physician screened the patient for internal cancers, especially ovarian cancer. Fortunately, the mammogram, Papanicolaou (Pap) smear, colonoscopy, transvaginal ultrasound for ovarian imaging, and abdominal/pelvic CT scans were all normal.

Introduction
Dermatomyositis is a rare, idiopathic inflammatory disease involving the striated muscles and the skin. The disease is characterized by progressive, symmetrical, proximal muscle weakness. Dermatologic manifestations may occur with or without muscular diseases and include the characteristic heliotrope rash (Figures 181-2, 181-3, 181-5, and 181-6), “shawl sign,” and Gottron papules of the PIP joints. Although primarily a disease of muscle and skin, dermatomyositis has a clear relationship with myocarditis and interstitial lung disease, as well as an increased risk of associated malignancy.
Figure 181-6

Classic heliotrope rash around the eyes of this 19-year-old woman newly diagnosed with dermatomyositis. The color “heliotrope” is a pink-purple tint named after the color of the heliotrope flower. As expected, her heliotrope rash is bilaterally symmetrical. This rash resolved on prednisone and hydroxychloroquine. (Courtesy of Richard P. Usatine, MD, and from Goodall J, Usatine RP. Skin rash and muscle weakness. J Fam Pract. 2005;54(10):864-868. Reproduced with permission from Frontline Medical Communications.)
Epidemiology
- Annual incidence of 5 to 8.9 per 1 million population.1
- Seen more commonly in women.1
- Can affect any age; however, it is more common in children and older adults.1
- Thirty-five percent to 40% of patients with dermatomyositis also have interstitial lung disease. It is the most common internal organ manifestation of the disease and greatly affects morbidity and mortality.1,2
- Has been linked to malignancy in up to 15% to 24% of adults.3
- Cancers most commonly associated are breast, ovary, lung, and GI tract. The most common type of cancer is adenocarcinoma. Ovarian cancer is overrepresented in those patients with dermatomyositis and cancer. Cancer is not typically seen in children with dermatomyositis.
- In adults, the presence of anti-p155 autoantibodies has shown to be strongly associated with malignancy, with a 27-fold increase in odds.4
Etiology and Pathophysiology
- Dermatomyositis is considered an autoimmune disease of unknown etiology. Environmental exposure and infectious agents may play a role in disease pathogenesis.
- Dermatomyositis has been shown to be a microangiopathy that affects the skin and muscle. The muscle weakness and skin manifestations may be a result of activation and deposition of complement, which cause lysis of endomysial capillaries and muscle ischemia.
Diagnosis
- Diagnosis includes 5 criteria: “definite” (skin findings plus any 3 of criteria 1 to 4), “probable” (skin findings plus 2 of any criteria 1 to 4), or “possible” (skin findings plus any 1 of criteria 1 to 4).2,5,6
- Proximal symmetric muscle weakness that progresses over weeks to months.
- Elevated serum levels of muscle enzymes (CK, AST, lactate dehydrogenase [LDH] and aldolase).
- Abnormal electromyogram.
- Abnormal muscle biopsy.
- Skin findings—Presence of cutaneous disease characteristic of dermatomyositis (heliotrope rash; Gottron papules are considered pathognomonic) (Figures 181-2, 181-3, 181-4, 181-5, 181-6, 181-7, and 181-8). Nonpathognomonic manifestations include malar erythema, and periungual and cuticular changes (Figure 181-9).
- Proximal symmetric muscle weakness that progresses over weeks to months.
- These criteria are still considered the “gold standard,” although they are old (1975) and currently under critical review because of several limitations. The criteria do not include specific autoantibodies or MRI findings.2,7,8
Figure 181-7
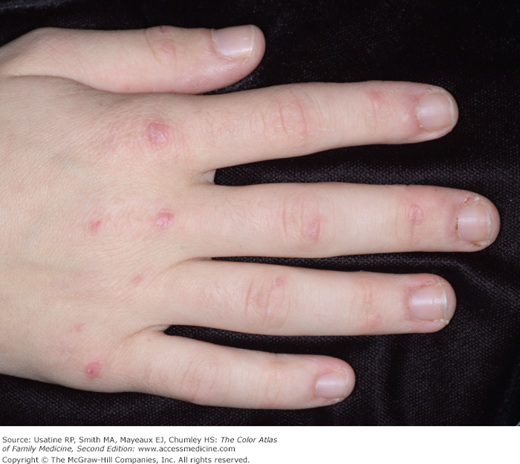
Hand involvement in the 19-year-old woman in Figure 181-6 with Gottron papules over the finger joints. She has nailfold erythema and ragged cuticles (Samitz sign). (Courtesy of Richard P. Usatine, MD, and from Goodall J, Usatine RP. Skin rash and muscle weakness. J Fam Pract. 2005;54(10):864-868. Reproduced with permission from Frontline Medical Communications.)
Figure 181-8

Juvenile dermatomyositis in a young boy. Note how the erythematous papules and plaques are most prominent over the finger joints and spare the space between joints. This is a good example of Gottron papules being very visible in juvenile dermatomyositis. (Courtesy of Richard P. Usatine, MD, and from Goodall J, Usatine RP. Skin rash and muscle weakness. J Fam Pract. 2005;54(10):864-868. Reproduced with permission from Frontline Medical Communications.)
Figure 181-9

Dermatomyositis in a man showing cuticular changes that are thick, rough, and hyperkeratotic with telangiectasias. This moth-eaten appearance of the cuticles is called the Samitz sign. The hands also have the appearance of “mechanic’s hands,” another sign seen in dermatomyositis. (Courtesy of the University of Texas Health Sciences Center, Division of Dermatology.)
Recent studies indicate that the dilated nailfold capillary loops (Figure 181-10) often seen in patients with dermatomyositis may help in earlier diagnosis and predicting patients with poor prognosis. Dilated nailfold capillary loops have shown promise in juvenile dermatomyositis as a marker for both skin and muscle disease activity to guide treatment. Some authors propose adding this finding to criteria for diagnosis.9,10
Figure 181-10

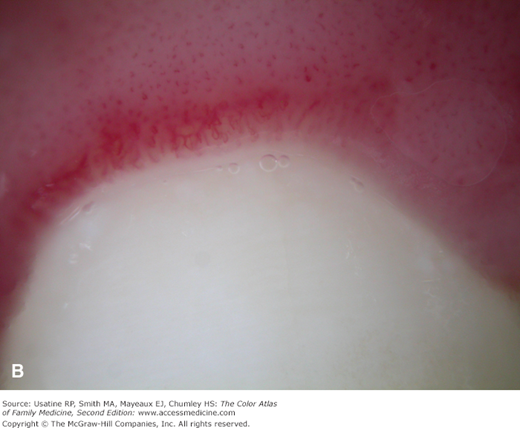

A. Dilated nailfold capillary loops visible with dermoscopy in a young woman with newly diagnosed dermatomyositis. B. She also had dilated capillary loops on the gingival borders of her teeth seen with dermoscopy. C. Marginal gingivitis in the same young woman with newly diagnosed dermatomyositis. The nailfold findings and gingival findings both resolved with treatment. (Courtesy of Richard P. Usatine, MD.)
- Bilateral periorbital heliotrope erythema (pathognomonic) (Figures 181-2, 181-3, 181-5, and 181-6) and scaling violaceous papular dermatitis in a patient complaining of proximal muscle weakness points to dermatomyositis.
- The patient may classically complain of difficulty climbing stairs, rising from a seat, or combing their hair. Notably the skin manifestations may precede, follow, or present simultaneously with muscle involvement; a patient may even have skin manifestations for longer than a year prior to developing muscle weakness.
- Hand involvement includes abnormal nailfolds and Gottron papules. “Moth-eaten” cuticles, also called the Samitz sign, are evidenced by periungual erythema and telangiectasias (Figures 181-7, 181-8, and 181-9).
- Gottron papules, smooth, purple-to-red papules and plaques, are classically located over the knuckles and on the sides of fingers (Figures 181-4

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


