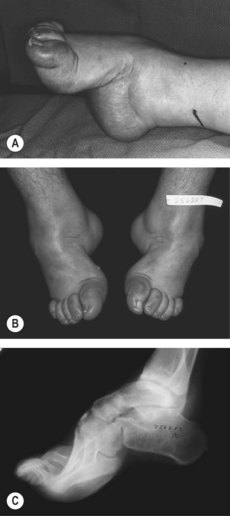
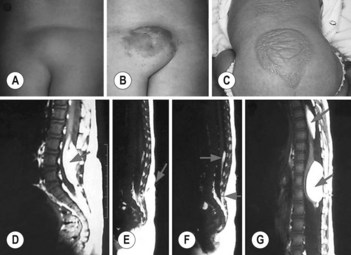
59 Deformity of a lower limb Instruction Examine the lower limbs of this patient who has had this abnormality since childhood. Salient features History • History of trauma to the spine and/or leg • History of poliomyelitis • History of weakness and fasciculations • Bladder and bowel symptoms. Examination • Wasting and deformity of one lower limb (or both with one side being more affected than the other) • Fasciculations • Normal tone in both lower limbs • Check the sensory system (L5 and/or S1 sensory loss in spina bifida) • Examine the spine: • Kyphoscoliosis (seen in poliomyelitis, indicating involvement of trunk muscles) • Tuft of hair in the lower lumbosacral spine (closed spina bifida). • Comment on bony deformity in the affected leg. Note: Always check the gait and test for Romberg’s sign. Diagnosis This patient has unilateral wasting and deformity of the R/L leg (lesion) caused by poliomyelitis in childhood (aetiology) and wears calipers on that leg (functional status). Questions What is the differential diagnosis? • Old poliomyelitis (Fig. 59.1) • Spina bifida (Fig. 59.2). Fig. 59.1 Medial (A) and frontal (B) views and radiograph (C) of severe calcaneocavovarus deformities as sequelae of poliomyelitis. (With permission from Canale, Beaty 2007.) Fig. 59.2 Clinical features and corresponding occult spinal dysraphism detected by sagittal, T1-weighted MRI studies of the spinal cord. (A) Sacral lipoma and deviated gluteal furrow. (B) Lumbar port-wine stain, lipoma, dermal sinus, and deviated gluteal furrow. (C) Dorsal and lumbar unclassified hamartomas. (D) Lipoma of the conus (arrow). (E) Dermal sinus (arrow). (F) Top of the lipoma of the filum terminale (upper arrow) and fistula (lower arrow). (G) Multiple lipomas of the thoracic cord (upper arrow) and posterior conus (lower arrow). (With permission from Guggisberg et al: 2004.) What are the causes of lower motor neuron signs in the legs? • Peripheral neuropathy • Prolapsed intervertebral disc • Diabetic amyotrophy • Poliomyelitis • Cauda equina lesions • Motor neuron disease. Only gold members can continue reading. Log In or Register to continue Share this: Share on X (Opens in new window) X Share on Facebook (Opens in new window) Facebook Like this:Like Loading... Related Related posts: Permanent cardiac pacemaker/implantable cardioverter-defibrillator Cauda equina syndrome Dermatomyositis Dystrophia myotonica Stay updated, free articles. Join our Telegram channel Join Tags: 250 Cases in Clinical Medicine Dec 4, 2016 | Posted by admin in GENERAL & FAMILY MEDICINE | Comments Off on Deformity of a lower limb Full access? Get Clinical Tree
59 Deformity of a lower limb Instruction Examine the lower limbs of this patient who has had this abnormality since childhood. Salient features History • History of trauma to the spine and/or leg • History of poliomyelitis • History of weakness and fasciculations • Bladder and bowel symptoms. Examination • Wasting and deformity of one lower limb (or both with one side being more affected than the other) • Fasciculations • Normal tone in both lower limbs • Check the sensory system (L5 and/or S1 sensory loss in spina bifida) • Examine the spine: • Kyphoscoliosis (seen in poliomyelitis, indicating involvement of trunk muscles) • Tuft of hair in the lower lumbosacral spine (closed spina bifida). • Comment on bony deformity in the affected leg. Note: Always check the gait and test for Romberg’s sign. Diagnosis This patient has unilateral wasting and deformity of the R/L leg (lesion) caused by poliomyelitis in childhood (aetiology) and wears calipers on that leg (functional status). Questions What is the differential diagnosis? • Old poliomyelitis (Fig. 59.1) • Spina bifida (Fig. 59.2). Fig. 59.1 Medial (A) and frontal (B) views and radiograph (C) of severe calcaneocavovarus deformities as sequelae of poliomyelitis. (With permission from Canale, Beaty 2007.) Fig. 59.2 Clinical features and corresponding occult spinal dysraphism detected by sagittal, T1-weighted MRI studies of the spinal cord. (A) Sacral lipoma and deviated gluteal furrow. (B) Lumbar port-wine stain, lipoma, dermal sinus, and deviated gluteal furrow. (C) Dorsal and lumbar unclassified hamartomas. (D) Lipoma of the conus (arrow). (E) Dermal sinus (arrow). (F) Top of the lipoma of the filum terminale (upper arrow) and fistula (lower arrow). (G) Multiple lipomas of the thoracic cord (upper arrow) and posterior conus (lower arrow). (With permission from Guggisberg et al: 2004.) What are the causes of lower motor neuron signs in the legs? • Peripheral neuropathy • Prolapsed intervertebral disc • Diabetic amyotrophy • Poliomyelitis • Cauda equina lesions • Motor neuron disease. Only gold members can continue reading. Log In or Register to continue Share this: Share on X (Opens in new window) X Share on Facebook (Opens in new window) Facebook Like this:Like Loading... Related Related posts: Permanent cardiac pacemaker/implantable cardioverter-defibrillator Cauda equina syndrome Dermatomyositis Dystrophia myotonica Stay updated, free articles. Join our Telegram channel Join Tags: 250 Cases in Clinical Medicine Dec 4, 2016 | Posted by admin in GENERAL & FAMILY MEDICINE | Comments Off on Deformity of a lower limb Full access? Get Clinical Tree