Cytopathology
Peter Kulesza
Isam A. Eltoum
▪ Questions and Answers
1. These nuclear changes (Fig. 2.1) are seen in thyroid papillary carcinoma and also in:
a. Lung carcinoma
b. Lymphoepithelial carcinomas
c. Rhabdoid tumor
d. Alveolar soft part sarcoma
e. Ewing sarcoma
View Answer
1. a. The presence of cytoplasmic nuclear inclusions is one of the features of papillary carcinoma but has been seen in other conditions of the thyroid, including Hashimoto thyroiditis and medullary carcinoma. It also has been reported in other non-thyroid diseases including lung carcinoma, melanoma, hemangioendotheliomas, hepatocellular carcinoma, pleomorphic adenoma, and other lesions as well.
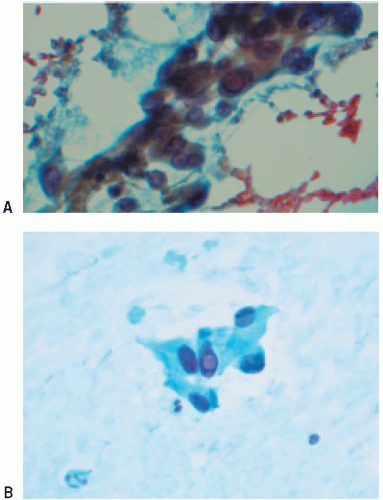 Figure 2.1 |
2. Conventional fluorescence in situ hybridization is useful in detection of all these conditions EXCEPT:
a. Demonstration of the number of chromosomes
b. Amplification of genes
c. Gene translocation
d. The number of cells in the S-phase of the cell cycle
e. Detection of viral genomes
View Answer
2. d. Fluorescence in situ hybridization does not detect the S-phase of the cell cycle. S-phase can be determined using flow cytometry.
3. In DNA content analysis using flow cytometry, which of the following statements is NOT correct?
a. Diploid content does not exclude malignancy.
b. Aneuploid content indicates malignancy.
c. Chromosomal translocations appear as a hyperdiploid peak.
d. Routine flow cytometry will not detect change of DNA content that is less than 2%.
e. DNA index reflects degree of tumor aneuploidy.
View Answer
3. c. A quantitative method of ploidy expression is the DNA index (DI), which is the ratio of the mean tumor cells at G0 /G1. The DNA content of normal diploid reference cells is 1. The greater the deviation of the DI from 1, the more “aneuploid” the tumor. Flow cytometry for DNA content does not detect chromosomal translocations. Translocations can be detected by FISH analysis or PCR for the chimeric gene or transcripts.
4. These cytologic changes (Fig. 2.2) are seen in all of these lesions EXCEPT:
a. Thyroid carcinoma
b. Ovarian carcinoma
c. Benign mesothelial lesions
d. Spindle cell melanoma
View Answer
4. d. These are psammoma bodies which are laminated calcific concretions seen frequently in papillary carcinomas including that of thyroid, ovary, endometrium, and kidney. They are commonly seen in meningiomas and in benign mesothelial hyperplasia. They are not known to occur in melanoma. Osteopontin protein has been reported to be involved in formation of psammoma bodies. Nanobacteria, a new controversial class of organisms, have been suggested as a possible cause.
5. Which of the following cytologic changes is NOT a common feature of adenocarcinoma?
a. Fine chromatin
b. Nuclear hyperchromasia
c. Prominent nucleoli
d. Mitosis
View Answer
5. b. Adenocarcinoma generally shows fine chromatin and sometimes chromatin clearing. The other listed features are common in adenocarcinoma.
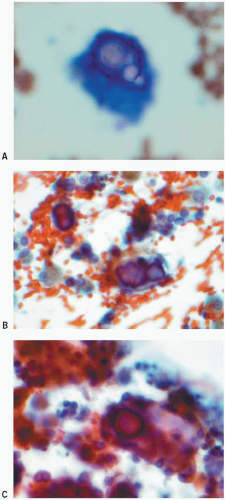 Figure 2.2 |
6. These cells (Fig. 2.3) are seen in pleural fluid in association with all of the following conditions EXCEPT:
a. Pneumothorax
b. Small lymphocytic lymphoma (SLL/CLL)
c. Blood in the pleural space
d. Hodgkin disease
e. Acute pulmonary embolism
View Answer
6. b. Pleural fluid eosinophilia is seen in pneumothorax, thoracentesis, pleural biopsy or surgery, introduction of blood in the pleural space (from infarction or trauma), and a few malignancies including Hodgkin disease. Pleural fluid eosinophilia is not a known feature of SLL/CLL.
7. Radiation therapy is often associated with all of the following cellular responses EXCEPT:
a. Vacuolated cytoplasm
b. Nuclear pleomorphism
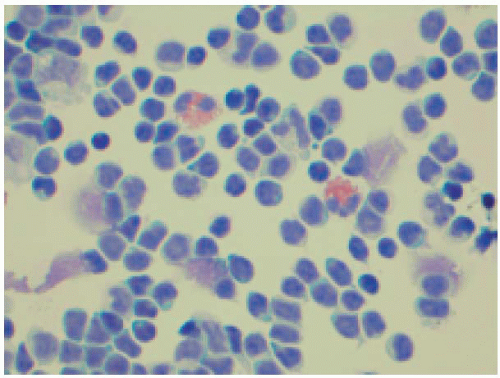 Figure 2.3 |
c. Prominent nucleoli
d. Hyperchromasia
e. High nuclear-cytoplasmic ratio
View Answer
7. d. Radiation can lead to numerous cellular changes including pleomorphism, nucleoli and hyperchromasia. Radiation is, however, associated with low nuclear- cytoplasmic ratio. This is one of the features that help differentiate it from dysplasia/neoplasia.
8. Increased numbers of lymphocytes in the pleural fluid are seen in:
a. Empyema
b. Pneumothorax
c. Systemic lupus erythematosus
d. Loeffler syndrome
e. Parasitic infestation
View Answer
8. c. Systemic lupus erythematosus is associated with pleural fluid lymphocytosis. Empyema causes neutrophilia, while Loeffler syndrome, parasites, and pneumothorax cause eosinophilia.
9. Bronchial cells in pleural fluid may be seen in all of the following conditions EXCEPT:
a. Bronchopleural fistula
b. Trauma
c. Price anomaly
d. Teratoma
e. Complication of bronchoscopy
View Answer
9. c. Price anomaly is a congenital disorder in which there is sequestration of part of the lung. It does not usually communicate with the pleural cavity. The other conditions are known to shed bronchial cells in the pleura.
10. All of the following are true about mesothelial cells EXCEPT:
a. The presence of ectoplasm and endoplasm is due to accumulation of organelles around the nucleus.
b. Windows are due to large microvilli.
c. Immunostains for calretinin does not differentiate between benign and malignant mesothelial lesions.
d. In pelvic washings, mesothelial cells have characteristically prominent nucleoli.
e. Immunostain with HBME-1 parallels calretinin in sensitivity but lacks specificity for mesothelial cells.
View Answer
10. d. In pelvic washing the mesothelial cells nuclei and nucleoli are not particularly prominent as these sells are not shed in an effusion which generally induces reactive changes including prominent nuclei and formation of cell balls.
11. Which of the following statements regarding fibrosarcomatous mesothelioma is true?
a. It is more likely to be associated with asbestos exposure than with epithelioid mesothelioma.
b. Diagnosis is more frequently established by fine needle aspiration than with fluid aspiration because it rarely presents as pleural effusion.
c. In spite of its name, the tumor is often formed of polygonal cells and is sometimes difficult to differentiate from metastatic non-small cell carcinoma.
d. The tumor is frequently CD34 positive and that helps differentiate it from other lesions that resemble it.
e. This tumor carries a better prognosis than epithelioid mesothelioma.
View Answer
11. b. This is a true mesothelial lesion and does not generally express CD34. This type of mesothelioma has the worst prognosis of all other histologic types. It can be confused with metastatic non-small cell carcinoma. This lesion does not shed cells in fluid.
12. Mesothelioma is NOT known to occur:
a. Following infection with SV40 in human
b. As a familial disease
c. Following occupational exposure
d. In childhood
e. In females
View Answer
12. a. Mesothelioma association with SV40 beyond doubt has not been established in humans.
13. This lesion (Fig. 2.4) is likely to have the following staining pattern in a cell block:
a. CEA+, EMA+, and MOC-31+
b. Vacuoles in the cytoplasm stain positively with oil red O but not with mucicarmine
c. Calretinin +, chromogranin +, and negative with synaptophysin
d. Calretinin +, mucicarmine +
e. Cytokeratin +, oil-red O +, and negative with calretinin
View Answer
13. b. This is true mesothelioma. Vacuoles in mesothelioma are positive for oil red O (which stains fat) but not mucicarmine (which stains mucin). Currently, calretinin, thrombomodulin, WT1 gene product, and keratin 5/6 are considered the best antibodies for the identification of mesothelial differentiation. It is generally advised that, in addition to positive “markers,” immunostaining panels should also include antibodies which should be negative in mesothelial cells and which may be positive in adenocarcinoma, particularly carcinoembryonic antigen (CEA), Ber EP4, Leu M1, MOC31, or B72.3
 Figure 2.4 |
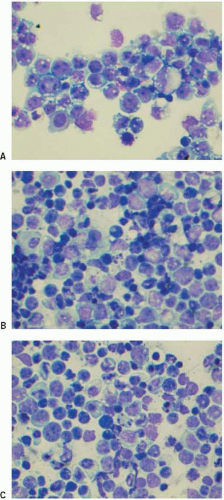 Figure 2.5 |
14. These are photomicrographs of a cytospin of a pleural fluid obtained from a 40-year-old man (Fig. 2.5). All the following viruses have been implicated in association with this lesion EXCEPT:
a. HSV-8
b. HIV
c. EBV
d. SV40
View Answer
14. d. This is a body-cavity based lymphoma. All the viruses listed, except SV40, have been implicated in the lesion.
15. Which of the following statements regarding intrapleural small round cell desmoplastic tumor is true?
a. Like Merkel cell tumors and small cell carcinoma, it often affects the elderly.
b. Desmoplasia is an essential element and needs to be present to differentiate this lesion from other small round cell tumors.
c. Individual cells are positive for desmin and cytokeratin.
d. Tumor cells are smaller than lymphocytes.
e. It has a characteristic EWS/Fli1 genomic translocation.
View Answer
15. c. Desmoplastic small round cell tumor of the pleura resembles that of intra-abdominal desmoplastic small round cell tumor and is positive for desmin and cytokeratin.
16. Features that are helpful to differentiate the above lesion from anaplastic large cell lymphoma include all of the following EXCEPT:
a. Visible amount of cytoplasm
b. Lymphoglandular bodies
c. Nuclear protrusion or cleavage
d. Prominent nucleoli
View Answer
16. a. Both have small but visible about of cytoplasm. The other features favor anaplastic large cell lymphoma.
17. Anaplastic large cell lymphoma stains with all the following markers EXCEPT:
a. CD45
b. CD30
c. ALK1
d. CD15
e. Epithelial membrane antigen (EMA)
18. This is a photomicrograph of a smear of peritoneal fluid obtained from a patient with ascites (Fig. 2.6). This lesion may be caused by all of the following tumors EXCEPT:
a. Ruptured mucinous cystadenoma of the appendix
b. Tumors of Meckel diverticulum
c. Lobular carcinoma of the breast
d. Mucinous tumor of the ovary
e. Tumors that express MUC2
View Answer
18. c. Pseudomyxoma peritoneii is caused by MUC2 mucin producing tumors, usually from the appendix or ovary. Lobular carcinoma of the breast is not known to be associated with pseudomyxoma peritoneii.
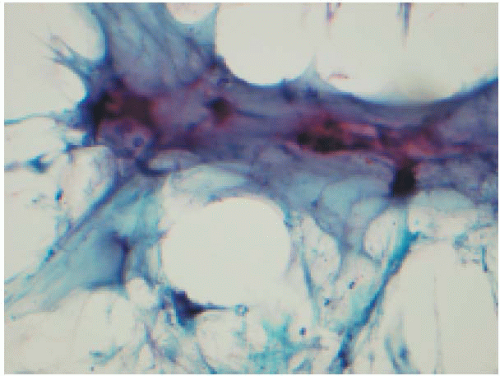 Figure 2.6 |
19. Features that are helpful in differentiating small lymphocytic lymphoma (SLL/CLL) from reactive lymphocytes in body fluid include all of the following, EXCEPT:
a. Massive apoptosis
b. High nuclear-cytoplasmic ratio
c. Monotony of cells
d. Conspicuous nucleoli
View Answer
19. b. High nuclear cytoplasm ratio is present in both conditions. The other features suggest small cell carcinoma.
20. In addition to the above features, CLL/SLL is positive for all of the following markers EXCEPT:
a. CD20
b. CD5
c. CD43
d. CD23
e. CD19
21. Which of the following statements about the cerebrospinal fluid (CSF) of neonates is true?
a. Lymphocytes are more frequent than monocytes.
b. The presence of choroid plexus is a normal finding.
c. The specimen should be rejected when there are numerous neutrophils.
d. Unlike in adults, cell block is the method of choice for processing CSF.
e. Eosinophils should not be normally present.
View Answer
21. d. Cell block is not a routine method for CSF. The material is usually not sufficient to be processed for cell block.
22. All of the following statements are true about fine needle aspiration (FNA) procedure EXCEPT:
a. Small-bore needle (high gauge) is better in obtaining specimens than large-bore needle.
b. The most common reason for a false-positive diagnosis is an attempt to make a diagnosis in unsatisfactory specimen.
c. The most common reason for a false-negative diagnosis is sampling error.
d. The material that is examined through core-needle biopsy is five times that of the material that is examined using FNA.
e. It can be performed under imaging guidance.
View Answer
22. a. To obtain a satisfactory specimen using FNA, small bore needle is better than large bore needle. Large bores (in excess of 23G) usually result in bleeding, which dilutes the specimen.
23. FNA is contraindicated in all of the following conditions EXCEPT:
a. Carotid-body tumor
b. Kaposi sarcoma
c. Pheochromocytoma
d. Echinococcus granulosus infection
e. Bleeding diathesis
View Answer
23. b. Kaposi sarcoma is not a contra-indication for FNA. Following FNA, carotid body tumor is known to be associated with thrombosis of carotid artery while pheochromocytoma may be followed by hypertensive crisis. Aspiration of an Echinococcus cyst (hydatid cyst) is known to be followed by anaphylaxis.
24. Which of the following statements about FNA procedure of the thyroid is true?
a. Patients are typically asked to swallow while the needle is inside the thyroid to make sure that the needle is in the lesion.
b. The needle is passed tangentially through the sternocleidomastoid muscle to avoid the great vessels.
c. The use of a large-bore needle ensures proper sampling.
d. In general, the best position for sampling is for the patient to lie flat without a pillow.
e. A lateral approach minimizes the risk of hematoma formation.
View Answer
24. d. The best position for the thyroid FNA is to let the patient lie flat without the pillow.
25. FNA of the breast has been largely replaced by the core biopsy; however, it is still used:
a. When the clinical and imaging suspicion is low
b. For a assessment of chromosome 3 amplification using FISH
c. For assessment of microcalcification
d. For ER/PR hormone assessment
e. When mammography shows a high-density lesion with spiculated appearance
View Answer
25. a. FNA is helpful when the clinical suspicion is low. Core biopsy is the preferred methods in the other three conditions.
26. This is a photomicrograph of an FNA of a subareolar nodule (Fig. 2.7). This lesion:
a. Is a metaplastic carcinoma with squamous cell component
b. Requires no further treatment
c. Arises in a lactiferous duct
d. Affects women only
e. Is fibrocystic disease
View Answer
26. c. This is subareolar abscess. It affects both men and women and does no heal without excision.
 Figure 2.7 |
27. These are photomicrographs of a smear of an FNA of the breast (Fig. 2.8). Each of the following is true about this lesion EXCEPT:
a. It increases the risk for developing breast cancer twofold.
b. It is frequently seen in a previous biopsy site.
c. Cells are positive for ER/PR but negative for Her2/neu.
d. It is can be clinically confused with cancer but the presence of foam cells is characteristic.
e. It occurs following trauma.
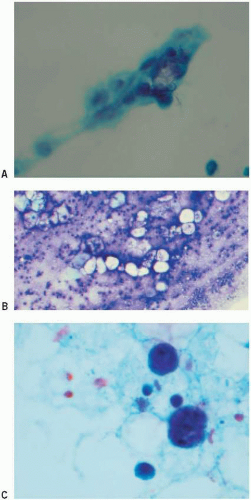 Figure 2.8 |
28. This is a photomicrograph of a smear of an FNA of the breast (Fig. 2.9). This type of tissue fragment is present in all of the following conditions EXCEPT:
a. Fibroadenoma
b. Fibrocystic change
c. Lobular carcinoma
d. Phyllodes tumor
View Answer
28. c. Smear of lobular carcinoma is usually associated with single cells. These are benign ductal cells and could be present in all of the other lesions.
 Figure 2.9 |
29. This is a photomicrograph of a smear of an FNA of the breast (Fig. 2.10). This lesion is most likely a:
a. Fibroadenoma
b. Fibrosis
c. Fibromatosis
d. Phyllodes tumor
e. Lobular carcinoma
View Answer
29. d. This is a fragment of stroma with few cells in between the fibers. The stromal fragments in phyllodes tumor are characteristically cellular fragments.
 Figure 2.10 |
30. This is a photomicrograph of a smear of an FNA of the breast (Fig. 2.11). This lesion is most likely a:
a. Tubular carcinoma
b. Ductal carcinoma
c. Lobular carcinoma
d. Mucinous carcinoma
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


