Cylindroma
Steven D. Billings, MD
Key Facts
Etiology/Pathogenesis
Familial cases associated with Brooke-Spiegler syndrome
Clinical Issues
Marked female predominance (F:M = 9:1)
90% present on head and neck
Microscopic Pathology
Dermal-based tumor, circumscribed but not encapsulated
Composed of multiple nodules/lobules of basaloid cells
Tumor lobules have complex pattern where they appear to fit together in a “jigsaw puzzle” pattern
Tumor lobules surrounded by dense eosinophilic basement membrane material
Lobules have 2 cell types: Small basaloid cells and larger pale cells
Focal ductal lumen formation
Globules of hyaline basement membrane material often present in interior of tumor nodules
Top Differential Diagnoses
Spiradenoma
Can have areas indistinguishable from cylindroma
Usually encapsulated
Tumor stroma has prominent vasculature
Malignant cylindroma/cylindrocarcinoma
Trichoblastoma
Tumor lobule surrounded by fibroblastic stroma; not thick basement membrane
Basal cell carcinoma
Peripheral palisading with tumor-stroma retraction
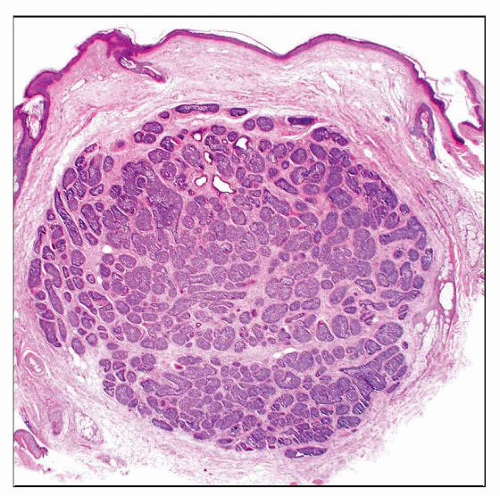 Cylindroma is typically a dermal-based, well-circumscribed, but unencapsulated tumor without connections to the overlying dermis. |
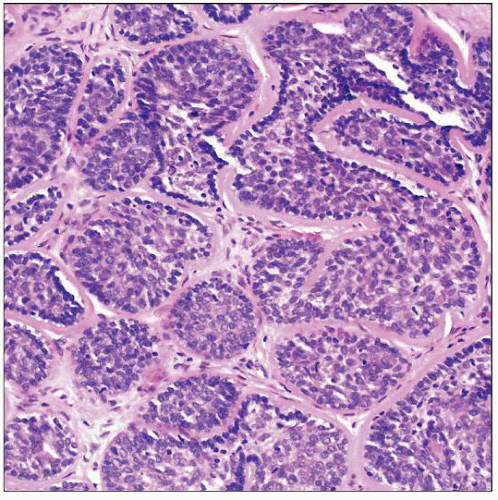 The tumor is composed of irregular lobules, surrounded by dense hyalinized membranous material, which appear to fit together in a pattern reminiscent of a jigsaw puzzle. |
TERMINOLOGY
Synonyms
Dermal cylindroma
Turban tumor (clinical term for multiple tumors on head)
Definitions
Benign dermal-based adnexal tumor with distinctive, “jigsaw puzzle” pattern
May show evidence of apocrine differentiation rather than eccrine differentiation in most cases
ETIOLOGY/PATHOGENESIS
Loss of Heterozygosity of Tumor Suppressor Gene CYLD
Mutation of CYLD found in both sporadic and familial cases
Sporadic or Familial
Familial cases associated with Brooke-Spiegler syndrome
Also known as familial cylindromatosis or turban tumor syndrome
Autosomal dominant
Predilection for women
Multiple eccrine spiradenomas and trichoepitheliomas often present as well
CLINICAL ISSUES
Epidemiology
Incidence
Common adnexal tumor of sweat glands
Age
Usually early adulthood
Gender
Marked female predominance (F:M = 9:1)
Site
90% present on head and neck
60% present on scalp
Presentation
Dermal mass
Treatment
Surgical approaches
Complete excision is curative
Prognosis
Benign; may recur if incompletely excised
Rare transformation to malignant cylindroma (cylindrocarcinoma), usually in large, longstanding tumors
MICROSCOPIC PATHOLOGY
Histologic Features
Usually located in upper dermis
No attachment to epidermis
Circumscribed but not encapsulated
Composed of multiple nodules/lobules of basaloid cells
Tumor lobules have complex pattern where tumor lobules appear to fit together in an irregular, “jigsaw puzzle” pattern
Tumor lobules surrounded by dense eosinophilic basement membrane material
Tumor lobules have 2 cell types
Outer, small basaloid cells with small hyperchromatic nuclei
Inner cells have larger oval nuclei with vesicular chromatin
Tumor cells positive for CK6, CK7, CK19, and EMA
Basaloid cells may be positive for SMA, calponin, and S100, consistent with myoepithelial differentiation
Focal ductal lumen formation
Lumina positive for CEA and EMA
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


