Cutaneous Malignant Fibrous Histiocytoma/Pleomorphic Sarcoma
Khin Thway, BSc, MBBS, FRCPath
Key Facts
Terminology
Anaplastic sarcoma composed of pleomorphic spindle and polygonal cells
No other definable differentiation, other than fibroblastic or myofibroblastic
Etiology/Pathogenesis
Small proportion of cases occur post irradiation or secondary to chronic ulceration/scarring
Clinical Issues
Most common adult soft tissue sarcoma
Older adults
Most frequent in deep soft tissue of extremities
Usually high-grade tumors
Superficial tumors have better prognosis than deep ones
Macroscopic Features
Thorough sampling required to demonstrate any possible line of differentiation
Heterogeneous cut surface
Necrosis and hemorrhage
Microscopic Pathology
Diagnosis of exclusion
Morphology shared by many tumors of different lineages
Storiform pattern, loose fascicles or sheets
Markedly atypical cells
Abundant mitoses and necrosis
No discernible microscopic features of differentiation
Immunohistochemical panel required to exclude tumors with specific differentiation
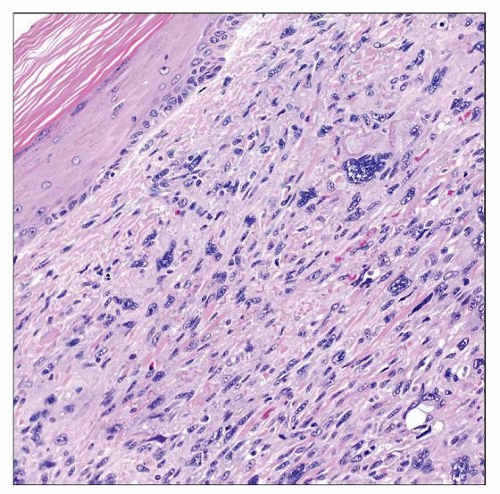 This cutaneous pleomorphic sarcoma is seen in the papillary dermis. Note the normal overlying epidermis without atypia or junctional activity, helping to exclude squamous cell carcinoma and melanoma. |
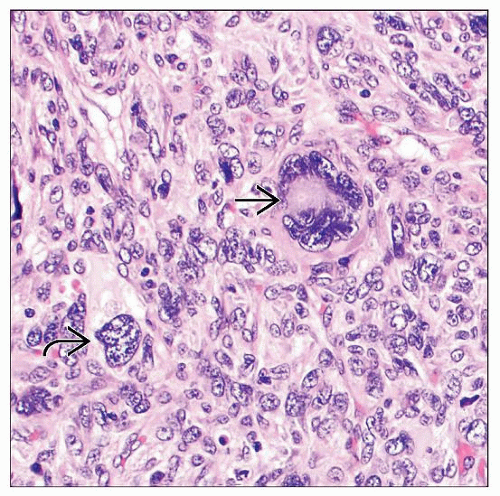 Microscopically, pleomorphic undifferentiated sarcoma is hypercellular with sheets of markedly anaplastic spindled and epithelioid cells, including bizarre  and multinucleated and multinucleated  forms. forms. |
TERMINOLOGY
Synonyms
Pleomorphic sarcoma
Undifferentiated high-grade sarcoma
Malignant fibrous histiocytoma (MFH)
Definitions
Anaplastic sarcoma composed of pleomorphic spindle and polygonal cells
No other definable differentiation, other than fibroblastic or myofibroblastic
Morphologic pattern shared by poorly differentiated or anaplastic tumors of different lineages
Diagnosis of pleomorphic sarcoma is therefore one of exclusion
ETIOLOGY/PATHOGENESIS
Environmental Exposure
Can occur at site of previous irradiation
Rarely secondary to chronic ulceration or scarring
CLINICAL ISSUES
Epidemiology
Incidence
Most common adult soft tissue sarcoma
Incidence increases with age
Age
Older adults
Very rare in adolescents and young adults
Gender
Slight male predominance
Site
Most are in deep soft tissue
Smaller numbers occur superficially in subcutaneous tissue
Dermal lesions are considered atypical fibroxanthoma (AFX) and have much better prognosis
Most in extremities (lower limb > upper limb)
May also arise on trunk
Presentation
Enlarging mass
Small proportion of patients have metastases at presentation
Prognosis
Usually high-grade tumors
Propensity for local recurrence and metastasis
Superficial tumors have better prognosis than deep ones
Myoid differentiation is prognostically adverse, with earlier metastasis
Applies whether differentiation is morphologic (leiomyosarcoma, myofibrosarcoma, rhabdomyosarcoma) or only immunohistochemical (actin, desmin)
MACROSCOPIC FEATURES
General Features
Lobulated
Generally circumscribed
Heterogeneous cut surface
Firm, solid, and softer myxoid areas
Necrosis and hemorrhage
Sections to Be Submitted
Thorough sampling required to demonstrate any possible line of differentiation
e.g., lipoblastic, muscle, epithelial
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


