Panniculitis but not in dermis or epidermis; lacks ulceration; TCRδ1(-), βF1(+)
Much better prognosis than CGDTCL
• Peripheral T-cell lymphoma, not otherwise specified
• Lupus profundus panniculitis
Similar inflammation in the subcutis in panniculitic pattern
Lobular panniculitis, but contains plasma cells and germinal centers, unlike CGDTCL
• Mycosis fungoides/pagetoid reticulosis
CGDTCL Presenting As an Ulcerated Mass Cutaneous γδ T-cell lymphoma (CGDTCL) shows a large raised lesion with ulcer and satellite lesions. (Courtesy C. Sander, MD.)
Primary CGDTCL Diffusely Involving Skin The atypical lymphoid infiltrate diffusely involves the epidermis , dermis , and also extended into the subcutaneous adipose tissue (not shown), typical of this neoplasm.
Panniculitis With Karyorrhexis In the same case, there is a deep infiltrate showing lobular panniculitis composed of atypical T cells rimming fat lobules with prominent apoptosis/karyorrhexis .
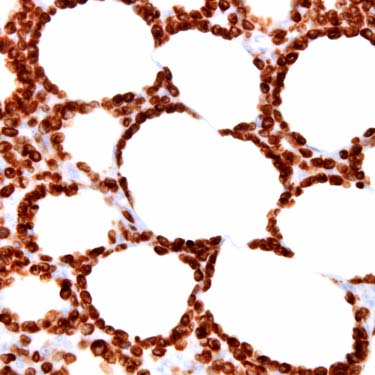
CD3 Immunohistochemical Stain in CGDTCL At high power, this CD3 stain highlights the atypical T cells that are lining fat cells. This feature is common to CGDTCL and to subcutaneous panniculitis-like T-cell lymphoma. (Courtesy L. J. Medeiros, MD.)
TERMINOLOGY
Abbreviations
• Cutaneous γδ T-cell lymphoma (CGDTCL)
Synonyms
• Subcutaneous panniculitis-like T-cell lymphoma with γδ cells
Definitions
• T-cell lymphoma arising in skin, which is composed of cytotoxic γδ T cells
Does not include subcutaneous panniculitis-like T-cell lymphoma composed of αβ cells
ETIOLOGY/PATHOGENESIS
Immunosuppression or Dysregulation of T Cells
• Found in many patients
Chronic Antigenic Stimulation
• Speculative but possibly involved in pathogenesis
Cell of Origin
• γδ T cells
Involved with mucosal and epithelial immune system function
CLINICAL ISSUES
Epidemiology
• Incidence
Rare tumor
– < 1% of all cutaneous T-cell lymphomas
• Age
Commonly adults
• Sex
No gender preponderance
Site
• Mostly extremities
Sometimes mucosal sites, where normal γδ T cells are found
Metastasis common
– Spread to lungs, liver, kidneys, oral mucosa, and brain
– Usually not in bone marrow, lymph nodes, or spleen
Presentation
• 1 or multiple skin lesions, sometimes with ulceration
• Patches due to epidermal infiltrates
Plaques or nodules due to dermal infiltrates
– ± ulcerated epidermis
• Hemophagocytic syndrome (HPS) may be present in 45% of cases
More often in subcutaneous lesions
– Related to release of cytotoxic molecules
• B symptoms are frequent
Laboratory Tests
• Cytopenias and ↑ liver function tests
• HHV8, HTLV-1, and EBV serologies (-)
Treatment
• Multiagent chemotherapy ± radiotherapy
Aggressive therapy followed by allogeneic allogenic stem cell transplant may be promising treatment modality
Brentuximab vedotin can be treatment option for patients with CD30(+) CGDTCL
Prognosis
• Poor prognosis
5-yr survival: ~ 11%; median survival: ~ 15 months
Subcutaneous disease is poor prognostic indicator
– Better prognosis if only disease in dermis or epidermis
HPS is poor prognostic indicator
May have indolent course in children
MICROSCOPIC
Histologic Features
• May involve epidermis, dermis, &/or subcutis
Epidermal
– Epidermotropism ranges from mild to marked
– Can mimic mycosis fungoides or pagetoid reticulosis
Dermal
– More dermal involvement typically present than in subcutaneous panniculitis-like T-cell lymphoma
Only gold members can continue reading. Log In or Register to continue






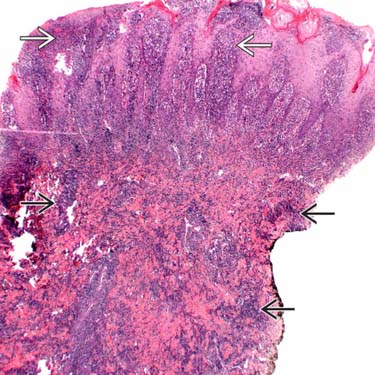
 , dermis
, dermis  , and also extended into the subcutaneous adipose tissue (not shown), typical of this neoplasm.
, and also extended into the subcutaneous adipose tissue (not shown), typical of this neoplasm.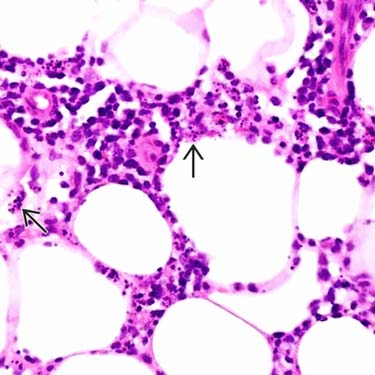
 .
.