3 Critical care and emergency medicine
A critically ill patient is one at imminent risk of death. The approach required in managing the critically ill patient differs from that required in less severely ill patients, with immediate resuscitation and stabilisation of the patient’s condition taking precedence. Intensive care units (ICUs) are for patients with potential or established organ failure. Initially established for the provision of mechanical ventilation for patients with respiratory failure, ICUs now monitor and support all the major organ systems. High-dependency care provides an intermediate level between intensive care and general ward care; it is appropriate for patients who have had major surgery and for those with single-organ failure.
Rigid rules to determine admission to ICU/HDU are destined to fail because every case must be evaluated on its own merits. The guiding principle when considering ICU/HDU admission should be the timely use of this resource in patients who have a realistic prospect of recovering to achieve a reasonable quality of life. Early identification and admission of critically ill patients improves survival and reduces the length of stay on the ICU (Box 3.1).
3.1 FACTORS IN THE ASSESSMENT OF A POSSIBLE ICU ADMISSION 
CLINICAL EXAMINATION OF THE CRITICALLY ILL PATIENT
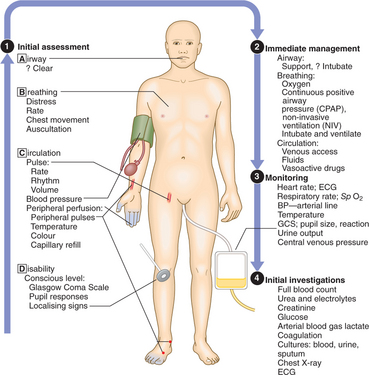
Recognising the critically ill patient
| Cardiovascular signs | Respiratory signs | Neurological signs |
|---|---|---|
MONITORING THE CIRCULATION
PRESENTING PROBLEMS
CIRCULATORY FAILURE: ‘SHOCK’
General features of shock are shown in Box 3.2.

RESPIRATORY FAILURE, INCLUDING ARDS
The majority of patients admitted to ICU/HDU will have respiratory problems either as the primary cause of their admission or secondary to pathology elsewhere. Attempts should be made to reduce the work of breathing, e.g. by treating bronchoconstriction or using continuous positive airways pressure (CPAP). The patient’s appearance (tachypnoea, difficulty speaking in complete sentences, laboured breathing, exhaustion, agitation or increasing obtundation) is more important than measurement of ABGs in deciding when to intubate and ventilate.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


