Cricothyroidotomy
Sam T. Windham III
DEFINITION
Cricothyroidotomy is an emergency procedure to establish airway access when orotracheal intubation is not possible or attempts have failed. As cricothyroidotomy has a high rate of complications compared to orotracheal intubation and tracheostomy, its role is limited to a rescue procedure for emergent airway access.
PATIENT HISTORY AND PHYSICAL FINDINGS
The circumstances surrounding the loss of airway are paramount to the use of cricothyroidotomy for establishment of the airway. These are broken down into patient-specific circumstances and setting-specific circumstances.
Patient-specific circumstances include trauma to face or upper airway, concern for cervical spine fractures, traumatic brain injury, limitations to cervical mobility, previous radiation to head and neck, and other circumstances leading to a difficult airway.
In certain circumstances such as potential isolated cervical spine fracture in a patient with a competent airway, attempts can be made to establish an airway by other means such as awake fiberoptic intubation or other intubation-assist devices.
In the setting of severe maxillofacial trauma where direct laryngoscopy is impeded by deranged anatomy, bleeding, and/or difficulty ventilating the patient, cricothyroidotomy should be considered early in the airway management algorithm.
Setting-specific circumstances also play a role as to the timing of emergency cricothyroidotomy in the airway algorithm. For example, considering the location where the airway is lost (such as the emergency department, operating room, or intensive care unit) will play a role in deciding what other options, equipment, and help are available.
If the loss of airway occurs in the operating room where full technical support is available, the full difficult airway algorithm may be used.1
The most common setting for the performance of cricothyroidotomy is for the trauma patient in an emergency room. In these patients with multiple injuries, suboptimal airway exposure due to need to maintain in-line cervical stabilization, and/or facial trauma, cricothyroidotomy should be prepared for at the first indication of a difficult airway.
SURGICAL MANAGEMENT
Preoperative Planning
Planning for the cricothyroidotomy begins before the situation arises, such as familiarization with the steps involved in the procedure and knowledge of the equipment available to perform the procedure.
Prepping the neck and obtaining equipment should begin with the second attempt of direct laryngoscopy in the difficult airway or at any sign of significant desaturation. Direct laryngoscopy may continue as the cricothyroidotomy is begun but should not delay the procedure. The pertinent anatomy and location of the cricothyroid membrane are illustrated in FIG 1.
Positioning
The patient is placed in the supine position with in-line cervical spine stabilization for trauma patients.
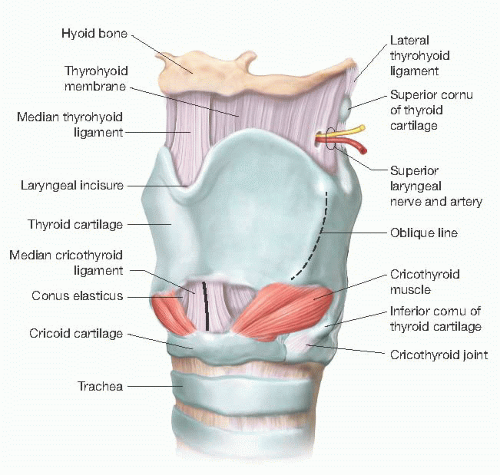 FIG 1 • Pertinent anatomy illustrating position of the cricothyroid membrane. |



