Q1: How can the company most clearly demonstrate that their new drug has a positive benefit-to-risk ratio in patients?
Q2: How can the company demonstrate that this new drug is as good as Drug X?
Q3: How can the company most clearly demonstrate that this new drug is better than Drug Y in safety and/or efficacy?
Q4: How can the company conduct clinical trials at a higher scientific standard than their competition, and thereby encourage regulatory agencies to require the other companies to redesign their trials at the new higher standard?
Q5: How can the company obtain “orphan drug status” and prevent other competing (identical) drugs from being marketed?
Q6: How can the company submit regulatory dossiers worldwide on a nearly simultaneous basis?
Q7: How can the company achieve regulatory approvals worldwide as rapidly as possible?
Q8: How can the company get its product to market most rapidly, both globally and in any particular developed country?
Q9: How can the company maximize the commercial returns from this product most rapidly?
Table 60.1 A few of the numerous considerations in creating a clinical development plan | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
distress syndrome. While it is not applicable (as a strategy) for all cases, it could be considered if there are competitors with similar or even identical drugs that are ahead or at the same state of development as the company. While this strategy can be attempted at any time, it is particularly effective if the company is first in a new indication.
Do my questions and responses make sense?
Have I considered all of the relevant factors?
Do the order and priority of questions make sense?
Will the strategy I am likely to create lead to obtaining data that will be the most relevant to achieve these goals?
If I substitute other questions and compare the responses and likely strategies will the answers seem less plausible? Take a “devil’s advocate” approach to improve one’s responses.
Use lateral thinking as a method (i.e., thinking “outside the box”) to see if you can derive other questions or another approach. (See books on lateral thinking by De Bono if this technique is unknown.)
Create a flow diagram, matrix or list to see which questions come before the others in sequence and to see which can (or should) be addressed simultaneously or additionally.
in development (i.e., ideal, realistic, desirable, minimally acceptable, or none) is a critical factor that will have a great influence on how the company pursues its chosen strategy. See Chapter 50 for a discussion on the types of standards that can be used.
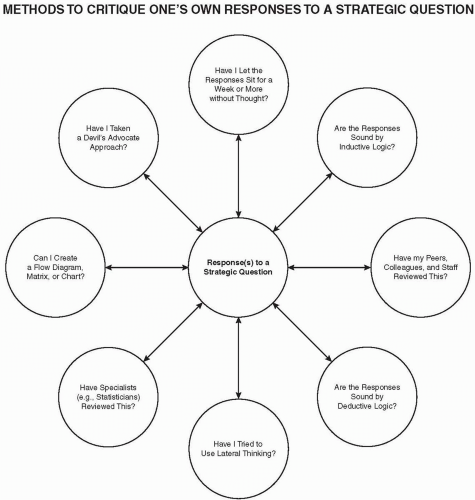 Figure 60.1 Methods to critique one’s own responses to a strategic question. |
Indication (i.e., disease) to be pursued. In some cases, this may not be known in detail. For example, new cancer treatments may identify two, three, or even more possible types of cancer (i.e., the indications), and they may be pursued simultaneously in Phase 2. The one where the greatest effect is observed is selected for additional studies.
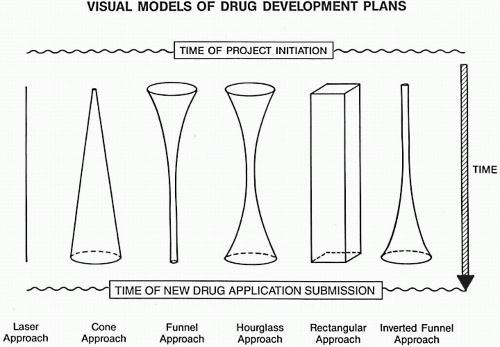
Figure 60.2 Illustrations of visual models of drug development.
Phase 1: No model is usually needed.
Phases 2 and 3: Use a single model for each drug.
Laser Approach
Uses one: indication, patient population, dosage form, route of administration, or dosing schedule
Cone Approach
The number of indications, patient populations, and dosage forms gradually increase during Phases 2 and 3.
Funnel Approach
Evaluating several indications or patient populations to choose one and focus development activities
Hourglass Approach
Evaluating several indications or patient populations to choose one and expand with several dosing schedules, patient populations, or dosage forms (e.g., in cancer drug development)
Rectangular or Cylinder Approach
A broad development plan is initiated from the outset.
Inverted Funnel Approach
Same as laser until the drug enters Phase 3a or 3b.
Phase 4: Using a model is optional; after approval for marketing, the same drug may reenter.
Phase 2: Use the same or a new model.
(Reprinted with permission from Spilker B. Guide to Clinical Trials. New York: Raven Press; 1991:878.)
Type of disease to be studied. For some diseases with multiple subtypes (e.g., epilepsy), it is usually critical to identify the specific subtype disease target to be selected. This is usually based on preclinical data.
Severity of disease to be studied. While it was previously mentioned that this is often unknown at the outset of a development program, it still is necessary to decide if the most appropriate (and commercially desirable) severity of patients
to treat is mild, moderate, or severe. While this is not critical or even appropriate for every disease, it is for most. One may also enroll patients of every severity in a trial (usually in Phase 2) to learn if there is a difference in their magnitude of response. However, it is often desirable or even necessary to stratify patients based on their severity to have balanced groups (e.g., in comparison with those given a placebo) to determine which group responds best to treatment.
Table 60.2 Questions to ask about studying the elderly in a clinical trial program
1.
Should elderly patients be studied in a separate trial or as part of trials in adults?
2.
Should pharmacokinetics be studied in the elderly?
3.
Are any precautions required for the elderly in studying this product?
4.
When during development should the elderly be studied, if at all?
5.
What are the regulatory issues and considerations about the elderly?
6.
Are there any theories or perspectives that need to be considered?
Dosage form(s) to initially study. While every company wishes that its new drug becomes a franchise with many dosage forms, packages, and indications, one usually begins development with a single dosage form. Occasionally, two dosage forms are studied from the outset. For example, it may be that the parenteral form is only studied initially to assure oneself that there are no issues with absorption when assessing efficacy, but the initial dosage form to be developed is the oral form. One of the regulatory and commercial issues often faced is that a parenteral form can reach the market more rapidly than an oral form, but will have a much smaller commercial market to compete in.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


