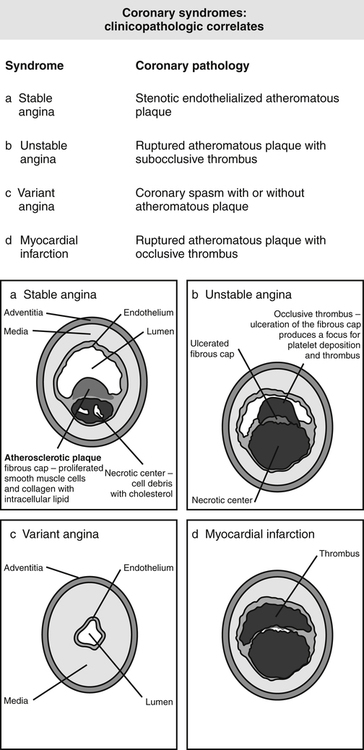
Chapter 18 Patients with a history of angina should have sublingual nitroglycerin (NTG) available, and they should know how to use it. Medications other than nitrates used to treat coronary artery disease (CAD) include β-blockers (BBs), calcium channel blockers (CCBs), angiotensin-converting enzyme inhibitors (ACEIs), ACE II inhibitors (ARBs), and antihyperlipidemics. Ranolazine is used in combination with some of these agents for patients with chronic angina. Use of these agents in the treatment of CAD is discussed here. Details on individual drugs are discussed in their respective chapters (Table 18-1). TABLE 18-1 Drugs Used for Coronary Artery Disease Discussed in Other Chapters The myocardium receives its blood supply from the coronary arteries, a system of small arteries that branch from the aorta (Figure 18-1). The right coronary artery lies in a groove between the right atrium and the right ventricle and supplies the right ventricle. The left main coronary artery is divided shortly after its origin into two branches: the left anterior descending branch and the circumflex branch. The left anterior descending branch supplies blood to the anterior myocardium, apex, and anterior septum and is located on the surface of the anterior myocardium. The circumflex branch lies in a groove between the left atrium and the left ventricle and supplies blood to the left ventricle. Smaller branches arise from the large coronary vessels. In 90% of the population, a posterior descending artery arises from the right coronary artery, and in 10%, it arises from the circumflex branch of the left anterior descending artery. Several large epidemiologic studies have identified certain habits and predisposing conditions that correlate with the development of CAD (Box 18-1). One can determine the 10-year coronary heart disease risk based on the Framingham study, as described by the National Cholesterol Education Program (NCEP) Expert Panel (see Chapter 24). • Stable or chronic angina is defined as no change in the past 2 months in terms of frequency, duration (<15 min), or precipitating causes. The symptom pattern is also reproducible. • Unstable angina is a change in pattern of pain such as an increase in frequency, severity, and/or duration of pain and fewer precipitating factors. Patients with unstable angina should be admitted to a coronary care unit. Treatment for unstable angina is beyond the scope of this text. Immediate care of the patient while hospitalization is awaited is discussed in the section on treatment guidelines. • Variant (Prinzmetal’s) angina refers to coronary artery spasm. This is very rare. Pain often occurs at rest and develops because of spasm rather than as the result of increased myocardial oxygen demand. • Silent ischemia is classified as asymptomatic episodes of myocardial ischemia that can be detected with the use of ECG and other diagnostic techniques. • Fraker TD Jr et al: 2007 chronic angina focused update of the ACC/AHA 2002 Guidelines for the management of patients with chronic stable angina: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines Writing Group to develop the focused update of the 2002 Guidelines for the management of patients with chronic stable angina, Circulation 116(23):2762-2772, 2007. • Canadian Cardiovascular Society; American Academy of Family Physicians; American College of Cardiology; American Heart Association; Antman EM et al: 2007 focused update of the ACC/AHA 2004 guidelines for the management of patients with ST-elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines, J Am Coll Cardiol 51(2):210-247, 2008. • Smith SC, Benjamin EJ, Bonow RO, et al: 2011 update of the AHA/ACCF secondary prevention and risk reduction therapy for patients with coronary and other atherosclerotic vascular disease: a guideline from the American Heart Association and American College of Cardiology Foundation Circulation 2011;124-2458-2473 or http://circ.ahajournals.org/content/early/2011/11/01/CIR.0b013e318235eb4d.citation. Accessed Feb 19, 2012. • Qaseem A, Fihn SD, Williams S, Dallas P, Owens DK, Shekelle P, and for the Clinical Guidelines Committee of the American College of Physicians. Diagnosis of stable ischemic heart disease: Summary of a clinical practice guidelines from the American College of Physicians/American College of Cardiology Foundation/American Heart Association/American Association for Thoracic Surgery/Preventive Cardiovascular Nurses Association/Society of Thoracic Surgeons. Annals of Internal Medicine Vol 157 No 10, 2013, pre-publication posting at http://annals.org/issue.aspx. • Stable angina, effective long-term single drug treatment regimens: antiplatelet drugs, β-blockers, calcium channel blockers, nitrates, potassium channel openers (ranolazine) • Unstable angina, beneficial or likely to be beneficial: aspirin, clopidogrel/ticlopidine
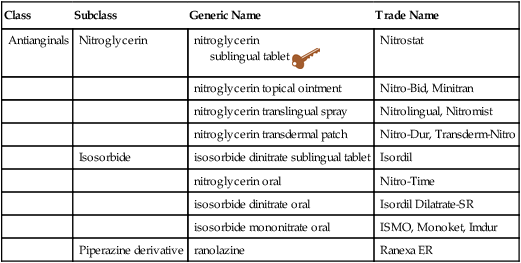
Coronary Artery Disease and Antianginal Medications
Class
Subclass
Generic Name
Trade Name
Antianginals
Nitroglycerin
nitroglycerin
sublingual tablet 
Nitrostat
nitroglycerin topical ointment
Nitro-Bid, Minitran
nitroglycerin translingual spray
Nitrolingual, Nitromist
nitroglycerin transdermal patch
Nitro-Dur, Transderm-Nitro
Isosorbide
isosorbide dinitrate sublingual tablet
Isordil
nitroglycerin oral
Nitro-Time
isosorbide dinitrate oral
Isordil Dilatrate-SR
isosorbide mononitrate oral
ISMO, Monoket, Imdur
Piperazine derivative
ranolazine
Ranexa ER
Class
Chapter
β-Blockers
20
Calcium channel blockers
21
ACE inhibitors
22
ACE II inhibitors
22
Antihyperlipidemics
24
Therapeutic Overview of Coronary Artery Disease
Anatomy and Physiology
Pathophysiology
Disease Process
Risk Factors
Classification
Treatment Principles
Standardized Guidelines
Evidence-Based Recommendations
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Coronary Artery Disease and Antianginal Medications

 Key drug. Sublingual nitroglycerin is selected as the key drug because it is the simplest form of the drug.
Key drug. Sublingual nitroglycerin is selected as the key drug because it is the simplest form of the drug.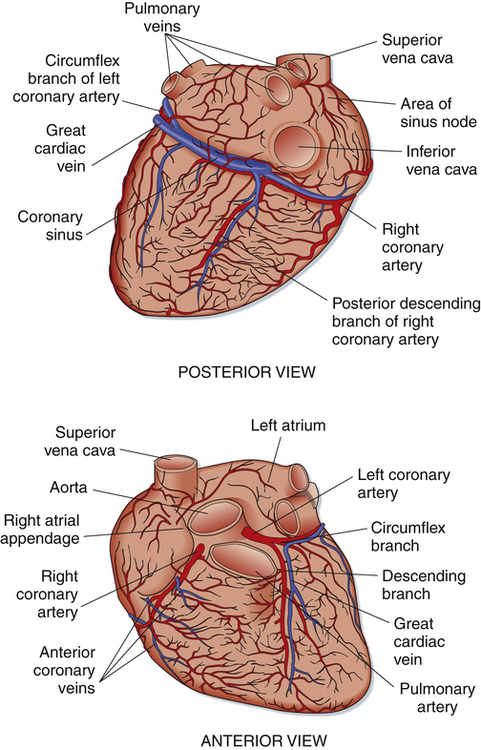
Only gold members can continue reading. Log In or Register to continue
