Patient Story
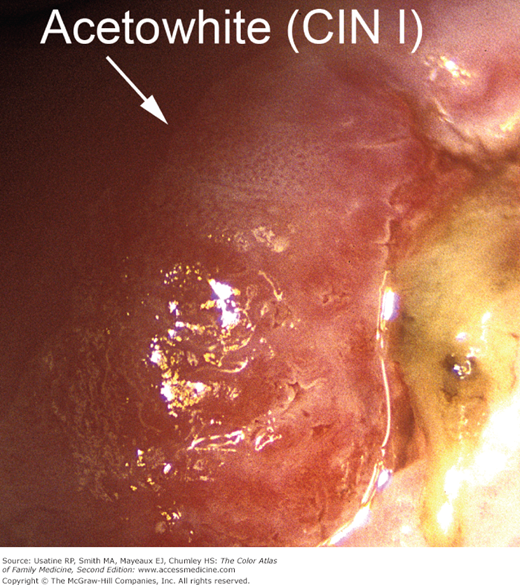
A 23-year-old woman has a low-grade squamous intraepithelial lesion on her Papanicolaou (Pap) test. One colposcopic view of her cervix shows acetowhite changes consistent with a cervical intraepithelial neoplasia grade 1 lesion (CIN 1) (Figure 89-1). She has no other suspicious findings and biopsy of the acetowhite area confirms CIN 1. The endocervical curettage is negative for disease. During the follow-up visit, the doctor and patient together decide to proceed with watchful waiting and repeat Pap tests at 6 and 12 months.
Introduction
Our knowledge of the genesis and development of cervical cancer has grown greatly over the last 20 years. It was once believed that human papillomavirus (HPV) infection and CIN 1 disease were the first steps in cancer formation. We now know that HPV infection and CIN 1 are essentially the same thing and will resolve without treatment in most immunocompetent women.
Epidemiology
- In low-grade squamous intraepithelial lesion (LGSIL) tests, the abnormalities are typically associated with HPV infection or CIN grade 1 lesions.1 Overall rates of Pap test abnormalities are often estimated from regional studies. For example, in an observational cohort study of routine cervical tests in the Northwest United States, in women of all ages (n = 150,052), atypical squamous cells was diagnosed at a rate of 9.8 per 1000, LGSIL was diagnosed at a rate of 3.5 per 1000, and negative routine tests occurred at a rate of 278.5 per 1000.2
Etiology and Pathophysiology
- Essentially all CIN is caused by HPV. Ten percent to 15% of CIN 1 lesions progress to CIN 2-3I, and 0.3% progress to cervical cancer.3
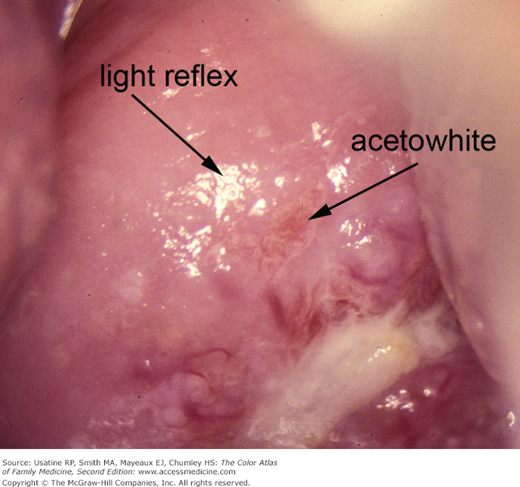
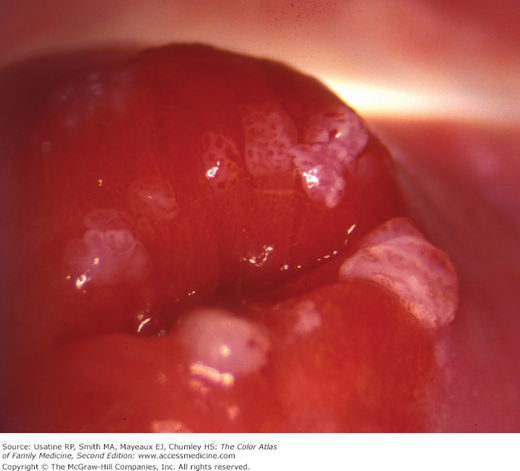
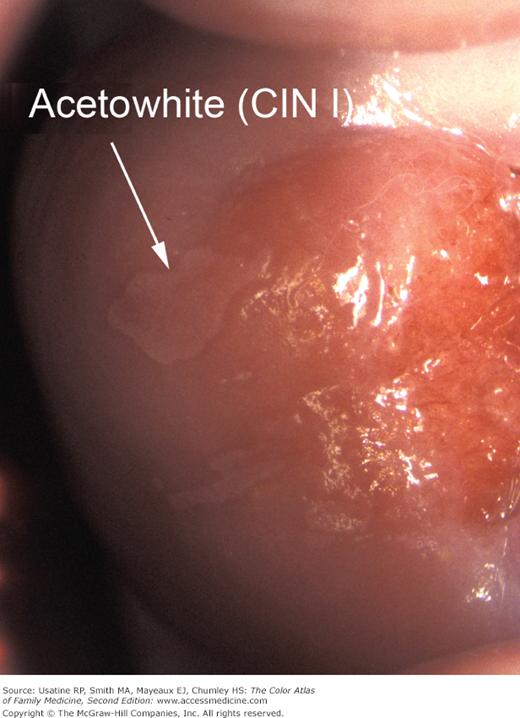
- There is no way to determine which CIN 1 lesions (Figures 89-1, 89-2, and 89-3) or simple HPV lesions (Figures 89-4 and 89-5) will regress or progress.
- Colposcopy is the standard of care for assessing abnormal Pap tests and cervical dysplasia. It entails the use of a field microscope to examine the cervix after acetic acid (Figures 89-1, 89-2, 89-3, and 89-4) and Lugol iodine (Figure 89-5.) Ten percent to 15% of CIN 1 lesions progress to CIN 2 or 3, and 0.3% progress to cervical cancer.3
- An atypical transformation zone is defined as a transformation zone with findings suggesting cervical dysplasia or neoplasia. Differences in thickness, density of the cells, degree of differentiation, and keratin production determine the color and opacity of the epithelium, and may produce the abnormal findings of leukoplakia and acetowhite epithelium.