Patient Story
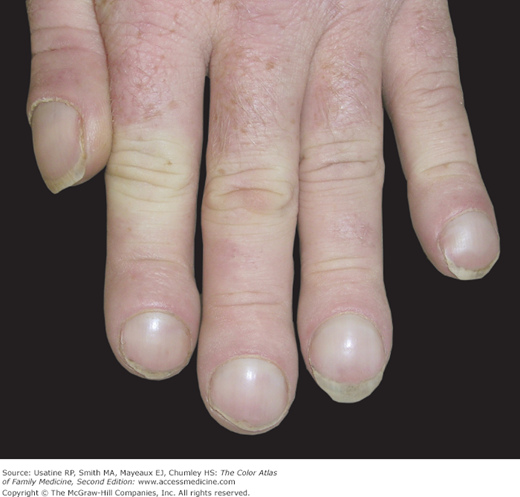
A 31-year-old man with congenital heart disease has had these clubbed fingers since his childhood (Figures 51-1 and 51-2). A close view of the fingers shows a widened club-like distal phalanx. He has learned to live with the limitations from his congenital heart disease and his fingers do not bother him at all.

Introduction
Clubbing is a physical examination finding first described by Hippocrates in 400 bc. Clubbing can be primary (pachydermoperiostosis or hypertrophic osteoarthropathy) or secondary (pulmonary, cardiac, or GI disease or HIV). Diagnosis is clinical based on nail fold angles and phalangeal depth ratios. The treatment is to correct the underlying cause, after which clubbing may resolve.
Epidemiology
- Two percent of adult patients admitted to a Welsh general medicine or surgery service.1
- Thirty-eight percent and 15% of patients with Crohn disease and ulcerative colitis, respectively.2
- Thirty-three percent and 11% of patients with lung cancer and chronic obstructive pulmonary disease (COPD), respectively.3
Etiology and Pathophysiology
- The etiology of clubbing is poorly understood.
- Increased connective tissue growth and angiogenesis in the nail bed result in the remodeling of the finger into a club shape.
- Current explanations include megakaryocyte release of platelet-activated growth factor, hypoxia, vasodilators in circulation, a neurocirculatory mechanism, and chronic activation of macrophages with production of profibrotic factors.4
Diagnosis
- History of present illness: Gradual onset of painless enlargement at the ends of the fingers and toes.
- Family history suggests primary hypertrophic osteoarthropathy/familial clubbing.
- Social history to identify exposure to asbestos, coal mine dust, and pigeons; tobacco use as risk factor for lung cancer; HIV and tuberculosis risk factors.
- Family history suggests primary hypertrophic osteoarthropathy/familial clubbing.
- Review of systems: Constitutional, pulmonary, GI, and musculoskeletal symptoms for clues to an underlying disease.5



