76 Carpal tunnel syndrome
Salient features
History
• Ask the patient about nocturnal pain (commonest cause of hand pain at night). Often the pain wakes up and shakes the hand to ameliorate symptoms: ‘wake and shake’.
• Pain, tingling, burning, numbness or some combination of these symptoms on the palmar aspect of the thumb, index finger, middle finger and radial half of the ring finger (no such symptoms affect the fifth finger even on detailed questioning).
• History of oral contraceptives, rheumatoid arthritis, myxoedema, acrogmegaly, chronic renal failure or sarcoidosis.
• Take a family history (abnormally small size of carpal tunnel runs in families).
Examination
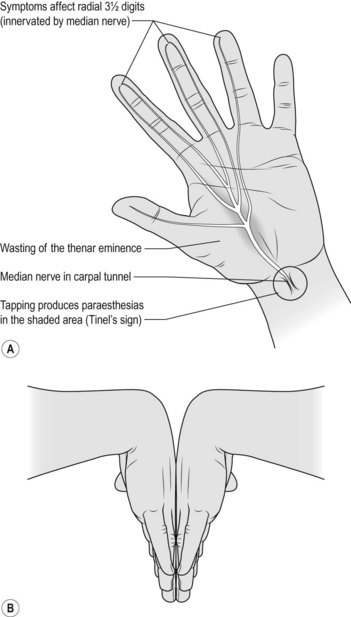
• Wasting of the thenar eminence (Fig. 76.1A)
• Weakness of flexion, abduction and opposition of thumb
• Diminished sensation over lateral three and half fingers
• Ask the patient, ‘What do you actually do with your hand(s) when symptoms are at their worst?’ If the patient makes flicking movement of the wrist and hand, similar to that employed in shaking down a clinical thermometer (the ‘flick sign’), this had both a sensitivity and a specificity >90% in one study (J Neurol Neurosurg Psychiatry 1984;47:870–2).
• Look carefully for scar of previous surgery (hidden by the crease of the wrist).
• Percuss over the course of the median nerve in the forearm: patient may experience tingling (Tinel’s sign (Fig. 76.1A). The sensitivity of Tinel’s sign ranges from 25 to 60%, although its specificity is higher (67 to 87%).
• Ask the patient to hyperextend the wrist maximally for 1 min; this may bring on symptoms (dysaesthesia over the thumb and lateral two and half fingers): Phalen’s test (Fig. 76.1B).
• Tell the examiner that you would like to:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


