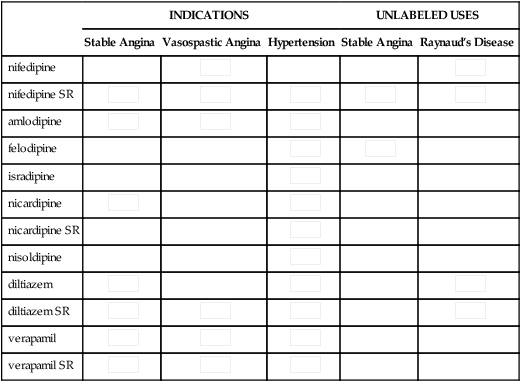
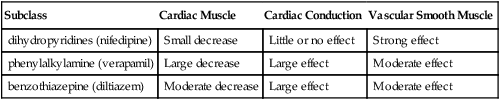
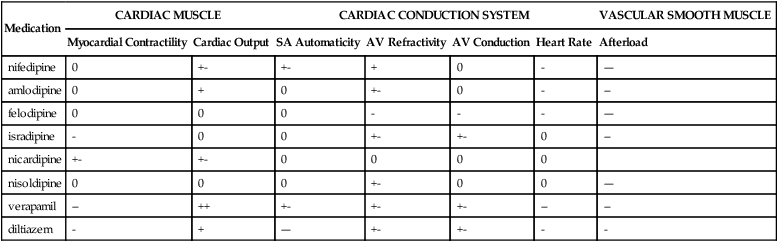
Chapter 21 INDICATIONS • Used off label for treatment of stable angina and Raynaud’s syndrome (Table 21-1) TABLE 21-1 Indications for and Unlabeled Uses of Calcium Channel Blockers Although these compounds have diverse chemical structures, they all share a basic electrophysiologic property: they block the inward movement of calcium through the slow channels of the cell membranes of cardiac and smooth muscle cells. The drugs differ in their location of action (Tables 21-2 and 21-3). The three types of tissue cells acted on are as follows: TABLE 21-2 Major Differences Between the Subclasses of Calcium Channel Blockers TABLE 21-3 Effect of Calcium Channel Blockers on Myocardium 1. Cardiac muscle (myocardium) 2. Cardiac conduction system: SA and AV nodes 3. Vascular smooth muscle: coronary arteries and arterioles, peripheral arterioles In these tissues, CCBs decrease automaticity in the SA node and decrease conduction in the AV node. Automaticity means that a cell depolarizes spontaneously and initiates an action potential without an external stimulus. Automaticity is a normal characteristic of SA nodal cells. Depolarization (Phase 0) of the action potential is normally generated by the inward calcium ion current through slow channels. Thus, agents that can block the inward calcium ion current across the cell membrane of SA nodal tissue decrease the rate of depolarization and depress automaticity. The result is a variable decrease in heart rate (a negative chronotropic effect) (Figure 21-1). Similarly, an agent that decreases calcium ion influx across the cell membrane of the AV node slows AV nodal conduction (negative chronotropic effect) and prolongs AV refractory time. When AV conduction is prolonged, fewer atrial impulses reach the ventricles, thus slowing the rate of ventricular contractions.
Calcium Channel Blockers
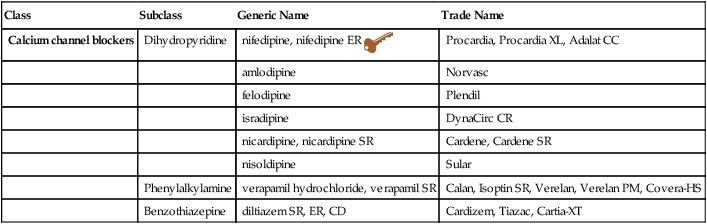
Class
Subclass
Generic Name
Trade Name
Calcium channel blockers
Dihydropyridine
nifedipine, nifedipine ER 
Procardia, Procardia XL, Adalat CC
amlodipine
Norvasc
felodipine
Plendil
isradipine
DynaCirc CR
nicardipine, nicardipine SR
Cardene, Cardene SR
nisoldipine
Sular
Phenylalkylamine
verapamil hydrochloride, verapamil SR
Calan, Isoptin SR, Verelan, Verelan PM, Covera-HS
Benzothiazepine
diltiazem SR, ER, CD
Cardizem, Tiazac, Cartia-XT
INDICATIONS
UNLABELED USES
Stable Angina
Vasospastic Angina
Hypertension
Stable Angina
Raynaud’s Disease
nifedipine


nifedipine SR





amlodipine



felodipine


isradipine

nicardipine


nicardipine SR

nisoldipine

diltiazem



diltiazem SR




verapamil



verapamil SR



Mechanism of Action
Subclass
Cardiac Muscle
Cardiac Conduction
Vascular Smooth Muscle
dihydropyridines (nifedipine)
Small decrease
Little or no effect
Strong effect
phenylalkylamine (verapamil)
Large decrease
Large effect
Moderate effect
benzothiazepine (diltiazem)
Moderate decrease
Large effect
Moderate effect
Medication
CARDIAC MUSCLE
CARDIAC CONDUCTION SYSTEM
VASCULAR SMOOTH MUSCLE
Myocardial Contractility
Cardiac Output
SA Automaticity
AV Refractivity
AV Conduction
Heart Rate
Afterload
nifedipine
0
+-
+-
+
0
–
—
amlodipine
0
+
0
+-
0
–
—
felodipine
0
0
0
–
–
–
—
isradipine
–
0
0
+-
+-
0
—
nicardipine
+-
+-
0
0
0
0
nisoldipine
0
0
0
+-
0
0
—
verapamil
—
++
+-
+-
+-
—
—
diltiazem
–
+
—
+-
+-
–
–
Cardiac Conduction System (SA and AV Nodes)
< div class='tao-gold-member'>
![]()
Stay updated, free articles. Join our Telegram channel

 Key drug.
Key drug. Short-acting nifedipine should not be used for the acute reduction of blood pressure, the control of essential hypertension, immediately after MI, or in acute coronary artery syndrome.
Short-acting nifedipine should not be used for the acute reduction of blood pressure, the control of essential hypertension, immediately after MI, or in acute coronary artery syndrome.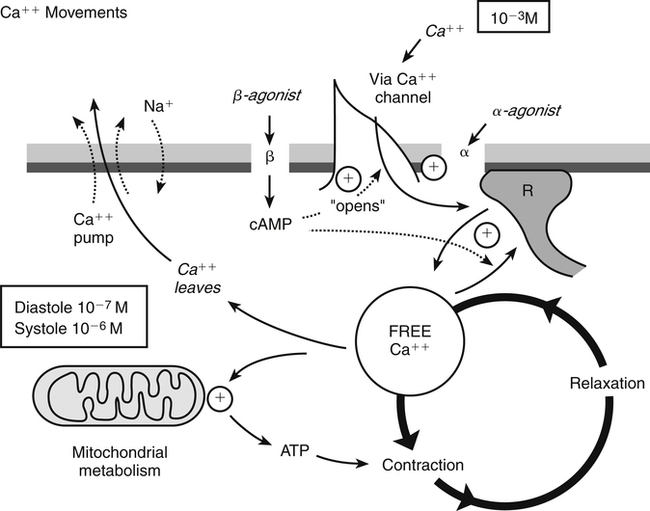

Full access? Get Clinical Tree


