EMERGENCY INTERVENTIONS
If you detect carpopedal spasm, quickly examine the patient for signs of respiratory distress (laryngospasm, stridor, loud crowing noises, cyanosis) or cardiac arrhythmias, which indicate hypocalcemia. Obtain blood specimens for electrolyte analysis (especially calcium and bicarbonate), and perform an electrocardiogram. Connect the patient to a cardiac monitor to watch for the appearance of arrhythmias. Administer an I.V. calcium preparation, and provide emergency respiratory and cardiac support. If calcium infusion doesn’t control seizures, administer a sedative, such as chloral hydrate or phenobarbital.
History and Physical Examination
If the patient isn’t in distress, obtain a detailed history. Ask about the onset and duration of the spasms and ask for a description of pain they produce. Also, ask about related signs and symptoms of hypocalcemia, such as numbness and tingling of the fingertips and feet, other muscle cramps or spasms, and nausea, vomiting, and abdominal pain. Check for previous neck surgery, calcium or magnesium deficiency, tetanus exposure, and hypoparathyroidism.
During the history, form a general impression of the patient’s mental status and behavior. If possible, ask family members or friends if they’ve noticed changes in the patient’s behavior. Mental confusion or even personality changes may occur with hypocalcemia.
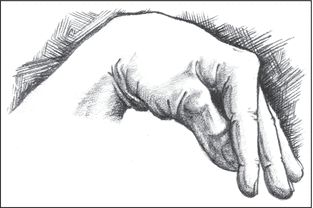
 EXAMINATION TIP Recognizing Carpopedal Spasm
EXAMINATION TIP Recognizing Carpopedal Spasm
In the hand, carpopedal spasm involves adduction of the thumb over the palm, followed by flexion of the metacarpophalangeal joints, extension of the interphalangeal joints (fingers together), adduction of the hyperextended fingers, and flexion of the wrist and elbow joints. Similar effects occur in the joints of the feet.
Inspect the patient’s skin and fingernails, noting dryness or scaling and ridged, brittle nails.
Medical Causes
- Hypocalcemia. Carpopedal spasm is an early sign of hypocalcemia. It’s usually accompanied by paresthesia of the fingers, toes, and perioral area; muscle weakness, twitching, and cramping; hyperreflexia; chorea; fatigue; and palpitations. Positive Chvostek’s and Trousseau’s signs can be elicited. Laryngospasm, stridor, and seizures may appear in severe hypocalcemia.
Chronic hypocalcemia may be accompanied by mental status changes; cramps; dry, scaly skin; brittle nails; and thin, patchy hair and eyebrows.
- Tetanus. Tetanus develops when Clostridium tetani enters a wound in a nonimmunized individual. The patient develops muscle spasms and painful seizures. Difficulty swallowing and a low-grade fever are also present. If the patient isn’t treated or treatment is delayed, the mortality rate is very high.
Other Causes
- Treatments. Multiple blood transfusions and parathyroidectomy may cause hypocalcemia, resulting in carpopedal spasm. Surgical procedures that impair calcium absorption, such as ileostomy formation and gastric resection with gastrojejunostomy, may also cause hypocalcemia.
Special Considerations
Carpopedal spasm can cause severe pain and anxiety, leading to hyperventilation. If this occurs, help the patient slow his breathing through your relaxing touch, reassuring attitude, and instructing him to breathe through pursed lips. Provide a quiet, dark environment to reduce his anxiety.
Prepare the patient for laboratory tests, such as complete blood count and serum calcium, phosphorus, and parathyroid hormone studies.
Patient Counseling
Explain the importance of tetanus immunization and keeping an immunization record and schedule.
Pediatric Pointers
Idiopathic hypoparathyroidism is a common cause of hypocalcemia in children. Carefully monitor children with this condition because carpopedal spasm may herald the onset of epileptiform seizures or generalized tetany followed by prolonged tonic spasms.
Geriatric Pointers
Always ask elderly patients about their immunization record. Suspect tetanus in anyone who comes to your facility with carpopedal spasm, difficulty swallowing, and seizures. Such patients may have incomplete immunizations or may not have had a recent booster shot. Always ask about any recent wound, no matter how inconsequential it may seem.
REFERENCES
McCormick, B. B., Davis, J., Burns, K. D. (2012). Severe hypocalcemia following denosumab injection in a hemodialysis patient. American Journal of Kidney Diseases, 60(4), 626–628.
Recker, R. R., Lewiecki, E. M., Miller, P. D., Reiffel, J. (2009). Safety of bisphosphonates in the treatment of osteoporosis. American Journal of Medicine, 122, S22–S32.
Cat’s Cry
Occurring during infancy, a mewing, kitten-like sound is the primary indicator of cat’s cry syndrome (also known as cri-du-chat). This syndrome affects about 1 in 50,000 neonates and causes profound mental retardation and failure to thrive. Most of those affected can have a normal life span; however, a few have serious organ defects and other life-threatening medical conditions.
 GENDER CUE
GENDER CUE
Cat’s cry syndrome affects females more commonly than males.
The chromosomal defect responsible (deletion of the short arm of chromosome 5) usually appears spontaneously, but may be inherited from a carrier parent. The characteristic cry is thought to result from abnormal laryngeal development. Associated features include microcephaly, low birth weight, distinctive facial features, and hypotonia.
 EMERGENCY INTERVENTIONS
EMERGENCY INTERVENTIONS
Suspect cat’s cry syndrome if you detect a kitten-like cry in a neonate. Be alert for signs of respiratory distress, such as nasal flaring; irregular, shallow respirations; cyanosis; and a respiratory rate over 60 breaths/minute. Be prepared to suction the neonate and to administer warmed oxygen. Keep emergency resuscitation equipment nearby because bradycardia may develop.
History and Physical Examination
Perform a physical examination, and note abnormalities. If you detect cat’s cry in an older infant, ask the parents when it developed. The sudden onset of an abnormal cry in an infant with a previously normal, vigorous cry suggests other disorders. (See “Cry, High-pitched”, pages 209 and 210.)
Medical Causes
- Cat’s cry syndrome. A kitten-like cry begins at birth or shortly thereafter. It’s accompanied by profound mental retardation, microcephaly, low birth weight, hypotonia, failure to thrive, and feeding difficulties. Typically, the neonate has a round face with wide-set eyes; strabismus; a broad-based nose with oblique or downsloping epicanthal folds; abnormally shaped, low-set ears; and an unusually small jaw. She may also have a short neck, webbed fingers, and a simian crease. Other abnormalities may include heart defects and GI abnormalities.
Special Considerations
Connect the neonate to an apnea monitor, and check for signs of respiratory distress. Keep suction equipment and warmed oxygen available. Obtain a blood sample for chromosomal analysis. Prepare the neonate for a computed tomography scan to rule out other causes of microcephaly and for an ear, nose, and throat examination to evaluate vocal cords.
Because the neonate with cat’s cry syndrome is usually a poor eater, monitor her intake, output, and weight.
Patient Counseling
Teach the parents about their child’s disorder and treatment options. Instruct the parents to offer the neonate small, frequent feedings. Prepare the parents to work long term with a team of specialists, such as those in genetics, neurology, cardiology, and speech and language. Discuss counselors or support groups that are available.
REFERENCES
Torun, D., Bahce, M., Alanbay, I., Guran, S., & Baser, I. (2009). Prenatal diagnosis of Cri-du chat syndrome following high maternal serum human chorionic gonadotropin and choroid plexus cysts. Prenatal Diagnosis, 29(5), 536–537.
Ye, Y., Luo, Y., Qian, Y., Xu, C., & Jin F. (2011). Cri du chat syndrome after preimplantation genetic diagnosis for reciprocal translocation. Fertility and Sterility, 96(1), e71–e75.
Chest Expansion, Asymmetrical
Asymmetrical chest expansion is the uneven extension of portions of the chest wall during inspiration. During normal respiration, the thorax uniformly expands upward and outward and then contracts downward and inward. When this process is disrupted, breathing becomes uncoordinated, resulting in asymmetrical chest expansion.
Asymmetrical chest expansion may develop suddenly or gradually and may affect one or both sides of the chest wall. It may occur as delayed expiration (chest lag), as abnormal movement during inspiration (for example, intercostal retractions, paradoxical movement, or chest-abdomen asynchrony), or as a unilateral absence of movement. This sign usually results from pleural disorders, such as life-threatening hemothorax or tension pneumothorax. (See Recognizing Life-threatening Causes of Asymmetrical Chest Expansion.) However, it can also result from a musculoskeletal or urologic disorder, airway obstruction, or trauma. Regardless of its underlying cause, asymmetrical chest expansion produces rapid and shallow or deep respirations that increase the work of breathing.
 EMERGENCY INTERVENTIONS
EMERGENCY INTERVENTIONS
If you detect asymmetrical chest expansion, first consider traumatic injury to the patient’s ribs or sternum, which can cause flail chest, a life-threatening emergency characterized by paradoxical chest movement. Quickly take the patient’s vital signs, and look for signs of acute respiratory distress — rapid and shallow respirations, tachycardia, and cyanosis. Use tape or sandbags to temporarily splint the unstable flail segment.
Depending on the severity of respiratory distress, administer oxygen by nasal cannula, mask, or mechanical ventilator. Insert an I.V. line to allow fluid replacement and administration of pain medication. Draw a blood sample from the patient for arterial blood gas analysis, and connect the patient to a cardiac monitor.
Although asymmetrical chest expansion may result from hemothorax, tension pneumothorax, bronchial obstruction, and other life-threatening causes, it isn’t a cardinal sign of these disorders. Because any form of asymmetrical chest expansion can compromise the patient’s respiratory status, don’t leave the patient unattended, and be alert for signs of respiratory distress.
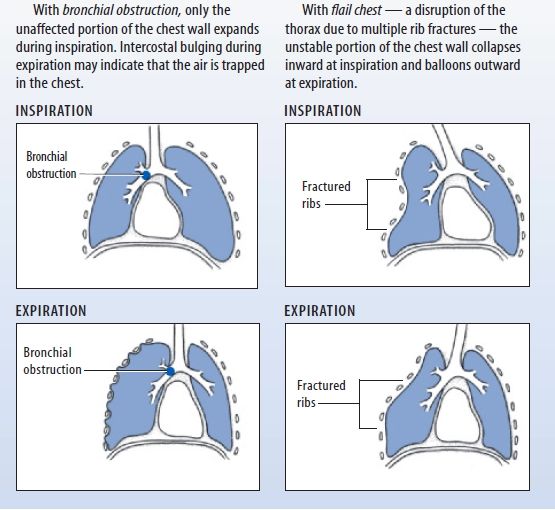
Recognizing Life-Threatening Causes of Asymmetrical Chest Expansion
Asymmetrical chest expansion can result from several life-threatening disorders. Two common causes — bronchial obstruction and flail chest — produce distinctive chest wall movements that provide important clues about the underlying disorder.
History and Physical Examination
If you don’t suspect flail chest and if the patient isn’t experiencing acute respiratory distress, obtain a brief history. Asymmetrical chest expansion commonly results from mechanical airflow obstruction, so find out if the patient is experiencing dyspnea or pain during breathing. If so, does he feel short of breath constantly or intermittently? Does the pain worsen his feeling of breathlessness? Does repositioning, coughing, or other activity relieve or worsen the patient’s dyspnea or pain? Is the pain more noticeable during inspiration or expiration? Can he inhale deeply?
Ask if the patient has a history of pulmonary or systemic illness, such as frequent upper respiratory tract infections, asthma, tuberculosis, pneumonia, or cancer. Has he had thoracic surgery? (This typically produces asymmetrical chest expansion on the affected side.) Also, ask about blunt or penetrating chest trauma, which may have caused pulmonary injury. Obtain an occupational history to find out if the patient may have inhaled toxic fumes or aspirated a toxic substance.
Next, perform a physical examination. Begin by gently palpating the trachea for midline positioning. (Deviation of the trachea usually indicates an acute problem requiring immediate intervention.) Then, examine the posterior chest wall for areas of tenderness or deformity. To evaluate the extent of asymmetrical chest expansion, place your hands — fingers together and thumbs abducted toward the spine — flat on both sections of the lower posterior chest wall. Position your thumbs at the 10th rib, and grasp the lateral rib cage with your hands. As the patient inhales, note the uneven separation of your thumbs, and gauge the distance between them. Then, repeat this technique on the upper posterior chest wall. Next, use the ulnar surface of your hand to palpate for vocal or tactile fremitus on both sides of the chest. To check for vocal fremitus, ask the patient to repeat “99” as you proceed. Note asymmetrical vibrations and areas of enhanced, diminished, or absent fremitus. Then, percuss and auscultate to detect air and fluid in the lungs and pleural spaces. Finally, auscultate all lung fields for normal and adventitious breath sounds. Examine the patient’s anterior chest wall, using the same assessment techniques.
Medical Causes
- Bronchial obstruction. Life-threatening loss of airway patency may occur gradually or suddenly. Typically, a lack of chest movement indicates complete obstruction; chest lag signals partial obstruction. If air is trapped in the chest, you may detect intercostal bulging during expiration and hyperresonance on percussion. You may also note dyspnea; accessory muscle use; decreased or absent breath sounds; and suprasternal, substernal, or intercostal retractions.
- Flail chest. With flail chest, a life-threatening injury to the ribs or sternum, the unstable portion of the chest wall collapses inward during inspiration and balloons outward during expiration (paradoxical movement). The patient may have ecchymoses, severe localized pain, or other signs of traumatic injury to the chest wall. He may also exhibit rapid, shallow respirations, tachycardia, and cyanosis.
- Hemothorax. Hemothorax is life-threatening bleeding into the pleural space that causes chest lag during inspiration. Other findings include signs of traumatic chest injury, stabbing pain at the injury site, anxiety, dullness on percussion, tachypnea, tachycardia, and hypoxemia. If hypovolemia occurs, you’ll note signs of shock, such as hypotension and a rapid, weak pulse.
- Kyphoscoliosis. Abnormal curvature of the thoracic spine in the anteroposterior direction (kyphosis) and the lateral direction (scoliosis) gradually compresses one lung and distends the other. This produces decreased chest wall movement on the compressed lung side and expands the intercostal muscles during inspiration on the opposite side. It can also produce ineffective coughing, dyspnea, back pain, and fatigue.
- Myasthenia gravis. Myasthenia gravis is a neuromuscular disease distinguished by varying degrees of weakness of voluntary muscles. The muscles that control breathing can be affected. Progressive loss of ventilatory muscle function produces asynchrony of the chest and abdomen during inspiration (“abdominal paradox”), which can lead to the onset of acute respiratory distress. Typically, the patient’s shallow respirations and increased muscle weakness cause severe dyspnea, tachypnea, and possible apnea.
- Pleural effusion. Chest lag at end-inspiration occurs gradually in this life-threatening accumulation of fluid, blood, or pus in the pleural space. Usually, some combination of dyspnea, tachypnea, and tachycardia precedes chest lag; the patient may also have pleuritic pain that worsens with coughing or deep breathing. The area of the effusion is delineated by dullness on percussion and by egophony, bronchophony, whispered pectoriloquy, decreased or absent breath sounds, and decreased tactile fremitus. A fever appears if infection causes the effusion.
- Pneumonia. Depending on whether fluid consolidation in the lungs develops unilaterally or bilaterally, asymmetrical chest expansion occurs as inspiratory chest lag or as chest-abdomen asynchrony. The patient typically has a fever, chills, tachycardia, tachypnea, and dyspnea along with crackles, rhonchi, and chest pain that worsens during deep breathing. He may also be fatigued and anorexic and have a productive cough with rust-colored sputum.
- Pneumothorax. Entrapment of air in the pleural space can cause chest lag at end-inspiration. Pneumothorax, a life-threatening condition, also causes sudden, stabbing chest pain that may radiate to the arms, face, back, or abdomen and dyspnea unrelated to the chest pain’s severity. Other findings include tachypnea, decreased tactile fremitus, tympany on percussion, decreased or absent breath sounds over the trapped air, tachycardia, restlessness, and anxiety.
With tension pneumothorax, the same signs and symptoms occur as in pneumothorax, but they’re much more severe. Tension pneumothorax rapidly compresses the heart and great vessels, causing cyanosis, hypotension, tachycardia, restlessness, and anxiety. The patient may also develop subcutaneous crepitation of the upper trunk, neck, and face, and mediastinal and tracheal deviation away from the affected side. You may auscultate a crunching sound over the precordium with each heartbeat; this indicates pneumomediastinum.
- Pulmonary embolism. Pulmonary embolism is an acute, life-threatening disorder that causes chest lag; sudden, stabbing chest pain; and tachycardia. The patient usually has severe dyspnea, blood-tinged sputum, a pleural friction rub, and acute anxiety.
Other Causes
- Treatments. Asymmetrical chest expansion can result from pneumonectomy and the surgical removal of several ribs. Chest lag or the absence of chest movement may also result from intubation of a mainstem bronchus, a serious complication typically due to the incorrect insertion of an endotracheal tube or movement of the tube while it’s in the trachea.
Special Considerations
If you’re caring for an intubated patient, regularly auscultate breath sounds in the lung peripheries to help detect a misplaced tube. If this occurs, prepare the patient for a chest X-ray to allow rapid repositioning of the tube. Because asymmetrical chest expansion increases the work of breathing, supplemental oxygen is usually given during acute events.
Patient Counseling
Explain to the patient or caregiver how to recognize early signs and symptoms of respiratory distress and what to do if they occur. Teach the patient coughing and deep breathing exercises and techniques that can help reduce anxiety.
Pediatric Pointers
Children have a greater risk than adults of mainstem bronchi (especially left bronchus) intubation. However, because children’s breath sounds are usually referred from one lung to the other because of the small size of the thoracic cage, use chest wall expansion as an indicator of correct tube position. Children also develop asymmetrical chest expansion, paradoxical breathing, and retractions with acute respiratory illnesses, such as bronchiolitis, asthma, and croup.
Congenital abnormalities, such as cerebral palsy and diaphragmatic hernia, can also cause asymmetrical chest expansion. With cerebral palsy, asymmetrical facial muscles usually accompany chest-abdomen asynchrony. With a life-threatening diaphragmatic hernia, asymmetrical expansion usually occurs on the left side of the chest.
Geriatric Pointers
Asymmetrical chest expansion may be more difficult to determine in this population because of the structural deformities associated with aging.
REFERENCES
Mohammad, A., Branicki, F., & Abu-Zidan, F. M. (2013). Educational and clinical impact of advanced trauma life support (ATLS) courses: A systematic review. World Journal of Surgery 38(2): 322–329.
Shere-Wolfe, R. F., Galvagno, S. M., & Grissom, T. E. (2012). Critical care considerations in the management of the trauma patient following initial resuscitation. Scandinavian Journal of Trauma and Resuscitative Emergency Medicine, 20, 68.
Chest Pain
Chest pain usually results from disorders that affect thoracic or abdominal organs — the heart, pleurae, lungs, esophagus, rib cage, gallbladder, pancreas, or stomach. An important indicator of several acute and life-threatening cardiopulmonary and GI disorders, chest pain can also result from a musculoskeletal or hematologic disorder, anxiety, and drug therapy.
Chest pain can arise suddenly or gradually, and its cause may be difficult to ascertain initially. The pain can radiate to the arms, neck, jaw, or back. It can be steady or intermittent, mild or acute. It can range in character from a sharp shooting sensation to a feeling of heaviness, fullness, or even indigestion. It can be provoked or aggravated by stress, anxiety, exertion, deep breathing, or eating certain foods.
 EMERGENCY INTERVENTIONS
EMERGENCY INTERVENTIONS
Ask the patient when his chest pain began. Did it develop suddenly or gradually? Is it more severe or frequent now than when it first started? Does anything relieve the pain? Does anything aggravate the pain? Ask the patient about associated symptoms. Sudden, severe chest pain requires prompt evaluation and treatment because it may herald a life-threatening disorder. (See Managing Severe Chest Pain, pages 154 and 155.)
History and Physical Examination
If the chest pain isn’t severe, proceed with the history. Ask if the patient feels diffuse pain or can point to the painful area. Sometimes a patient won’t perceive the sensation he’s feeling as pain, so ask whether he has any discomfort radiating to his neck, jaw, arms, or back. If he does, ask him to describe it. Is it a dull, aching, pressure-like sensation? Is it a sharp, stabbing, knifelike pain? Does he feel it on the surface or deep inside? Find out whether it’s constant or intermittent. If it’s intermittent, how long does it last? Ask if movement, exertion, breathing, position changes, or eating certain foods worsens or helps relieve the pain. Does anything in particular seem to bring it on?
Review the patient’s history for cardiac or pulmonary disease, chest trauma, intestinal disease, or sickle cell anemia. Find out which medications he’s taking, if any, and ask about recent dosage or schedule changes.
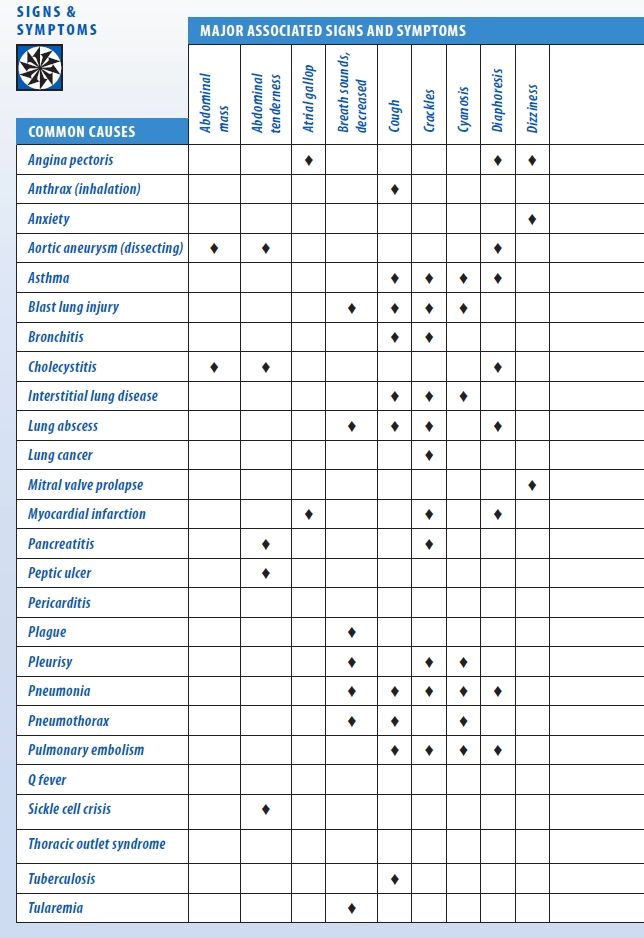
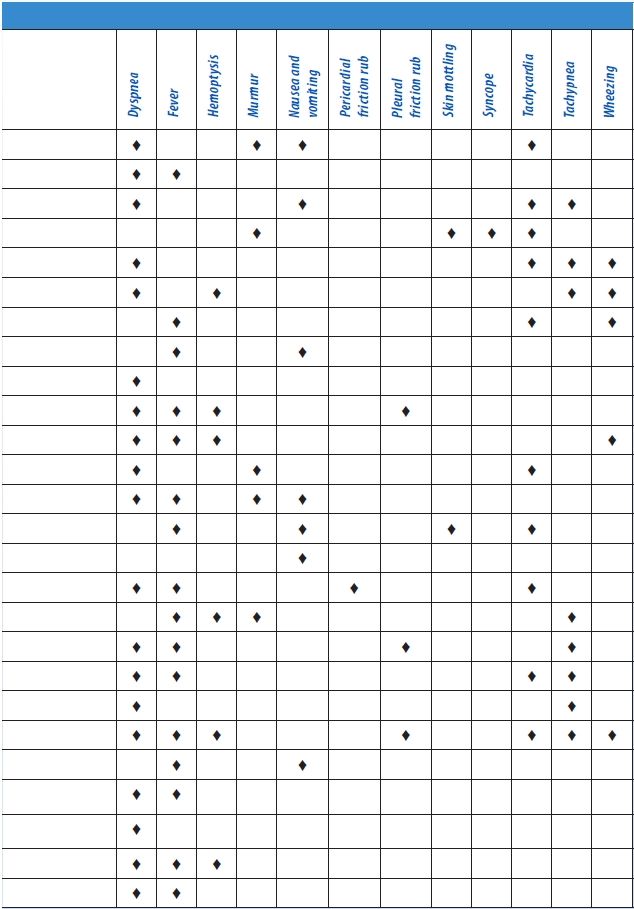
Take the patient’s vital signs, noting tachypnea, fever, tachycardia, oxygen saturation, paradoxical pulse, and hypertension or hypotension. Also, look for jugular vein distention and peripheral edema. Observe the patient’s breathing pattern, and inspect his chest for asymmetrical expansion. Auscultate his lungs for pleural friction rub, crackles, rhonchi, wheezing, or diminished or absent breath sounds. Next, auscultate for murmurs, clicks, gallops, or pericardial friction rubs. Palpate for lifts, heaves, thrills, gallops, tactile fremitus, and abdominal masses or tenderness. (See Chest Pain: Common Causes and Associated Findings, pages 156 and 157.)
Medical Causes
- Angina pectoris. With angina pectoris, the patient may experience a feeling of tightness or pressure in the chest that he describes as pain or a sensation of indigestion or expansion. The pain usually occurs in the retrosternal region over a palm-sized or larger area. It may radiate to the neck, jaw, and arms — classically, to the inner aspect of the left arm. Angina tends to begin gradually, build to its maximum, and then slowly subside. Provoked by exertion, emotional stress, or a heavy meal, the pain typically lasts 2 to 10 minutes (usually no longer than 20 minutes). Associated findings include dyspnea, nausea, vomiting, tachycardia, dizziness, diaphoresis, belching, and palpitations. You may hear an atrial gallop (a fourth heart sound) or murmur during an anginal episode.
With Prinzmetal’s angina, caused by vasospasm of coronary vessels, chest pain typically occurs when the patient is at rest — or it may awaken him. It may be accompanied by shortness of breath, nausea, vomiting, dizziness, and palpitations. During an attack, you may hear an atrial gallop.
- Anthrax (inhalation). Anthrax is an acute infectious disease that’s caused by the gram-positive, spore-forming bacterium Bacillus anthracis. Although the disease most commonly occurs in wild and domestic grazing animals, such as cattle, sheep, and goats, the spores can live in the soil for many years. The disease can occur in humans exposed to infected animals, tissue from infected animals, or biological warfare. Most natural cases occur in agricultural regions worldwide. Anthrax may occur in a cutaneous, inhalation, or GI form.
Inhalation anthrax is caused by inhalation of aerosolized spores. Initial signs and symptoms are flulike and include a fever, chills, weakness, a cough, and chest pain. The disease generally occurs in two stages with a period of recovery after the initial signs and symptoms. The second stage develops abruptly with rapid deterioration marked by a fever, dyspnea, stridor, and hypotension, generally leading to death within 24 hours. Radiologic findings include mediastinitis and symmetric mediastinal widening.
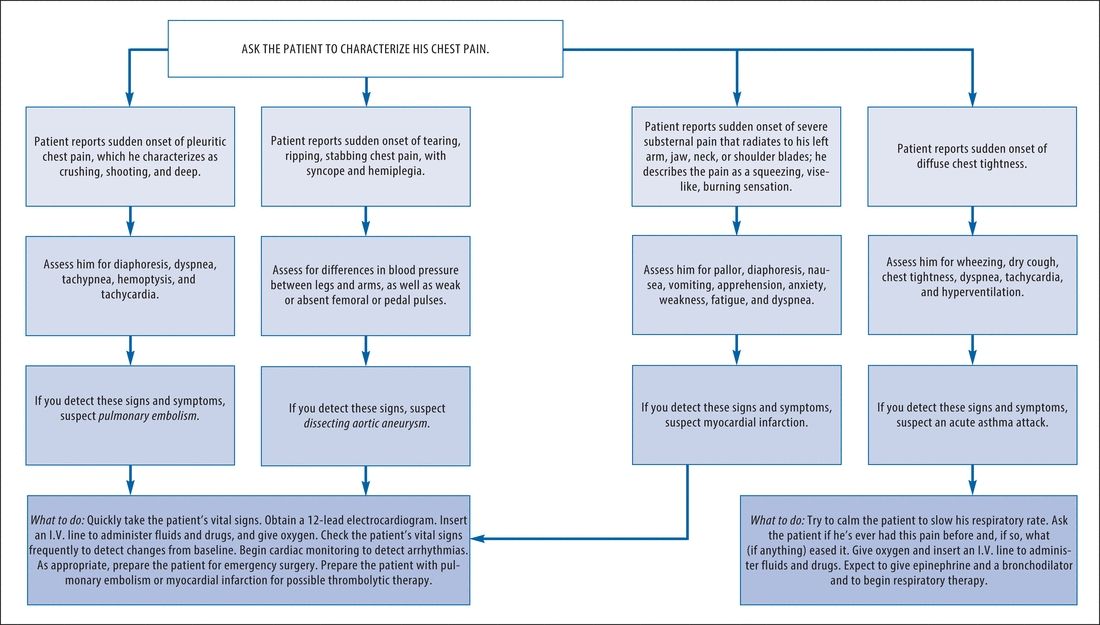
Managing Severe Chest Pain
Sudden, severe chest pain may result from any one of several life-threatening disorders. Your evaluation and interventions will vary, depending on the pain’s location and character. This flowchart will help you establish priorities for managing this emergency successfully.
Chest Pain: Common Causes and Associated Findings
- Anxiety. Acute anxiety — or, more commonly, panic attacks — can produce intermittent, sharp, stabbing pain, commonly located behind the left breast. This pain isn’t related to exertion and lasts only a few seconds, but the patient may experience a precordial ache or a sensation of heaviness that lasts for hours or days. Associated signs and symptoms include precordial tenderness, palpitations, fatigue, a headache, insomnia, breathlessness, nausea, vomiting, diarrhea, and tremors. Panic attacks may be associated with catastrophic events or agoraphobia — the fear of leaving home or being in open places with other people.
- Aortic aneurysm (dissecting). The chest pain associated with a dissecting aortic aneurysm usually begins suddenly and is most severe at its onset. The patient describes an excruciating tearing, ripping, stabbing pain in his chest and neck that radiates to his upper back, abdomen, and lower back. He may also have abdominal tenderness, a palpable abdominal mass, tachycardia, murmurs, syncope, blindness, loss of consciousness, weakness or transient paralysis of the arms or legs, a systolic bruit, systemic hypotension, asymmetrical brachial pulses, a lower blood pressure in the legs than in the arms, and weak or absent femoral or pedal pulses. His skin is pale, cool, diaphoretic, and mottled below the waist. Capillary refill time is increased in the toes, and palpation may reveal decreased pulsation in one or both carotid arteries.
- Asthma. In a life-threatening asthma attack, diffuse and painful chest tightness arises suddenly along with a dry cough and mild wheezing, which progress to a productive cough, audible wheezing, and severe dyspnea. Related respiratory findings include rhonchi, crackles, prolonged expirations, intercostal and supraclavicular retractions on inspiration, accessory muscle use, flaring nostrils, and tachypnea. The patient may also experience anxiety, tachycardia, diaphoresis, flushing, and cyanosis.
- Blast lung injury. Resulting from a gust wave after a high explosion discharges upon the body, blast lung injury causes severe chest pain, skin tears, contusions, edema, and hemorrhage of the lungs. Associated respiratory findings include dyspnea, hemoptysis, cough, tachypnea, hypoxia, wheezing, apnea, cyanosis, decreased breath sounds, and hemodynamic instability. Global acts of terrorism have increased the incidence of this condition. Chest X-rays, arterial blood gas measurements, computerized tomography scans, and Doppler technology are common diagnostic tools. There are no definitive guidelines for caring for those with blast lung injury; treatment is based on the nature of the explosion, the environment in which it occurred, and any chemical or biological agents involved.
- Bronchitis. In its acute form, bronchitis produces a burning chest pain or a sensation of substernal tightness. It also produces a cough, initially dry but later productive, that worsens the chest pain. Other findings include a low-grade fever, chills, a sore throat, tachycardia, muscle and back pain, rhonchi, crackles, and wheezing. Severe bronchitis causes a fever of 101°F to 102°F (38.3°C to 38.9°C) and possible bronchospasm with worsening wheezing and increased coughing.
- Cholecystitis. Cholecystitis typically produces abrupt epigastric or right upper quadrant pain, which may be sharp or intensely aching. Steady or intermittent pain may radiate to the back or right shoulder. Commonly associated findings include nausea, vomiting, a fever, diaphoresis, and chills. Palpation of the right upper quadrant may reveal an abdominal mass, rigidity, distention, or tenderness. Murphy’s sign — inspiratory arrest elicited when the examiner palpates the right upper quadrant as the patient takes a deep breath — may also occur.
- Interstitial lung disease. As interstitial lung disease advances, the patient may experience pleuritic chest pain along with progressive dyspnea, cellophane-type crackles, a nonproductive cough, fatigue, weight loss, decreased exercise tolerance, clubbing, and cyanosis.
- Lung abscess. Pleuritic chest pain develops insidiously in lung abscess along with a pleural friction rub and a cough that raises copious amounts of purulent, foul-smelling, blood-tinged sputum. The affected side is dull to percussion, and decreased breath sounds and crackles may be heard. The patient also displays diaphoresis, anorexia, weight loss, a fever, chills, fatigue, weakness, dyspnea, and clubbing.
- Lung cancer. The chest pain associated with lung cancer is commonly described as an intermittent aching felt deep within the chest. If the tumor metastasizes to the ribs or vertebrae, the pain becomes localized, continuous, and gnawing. Associated findings include cough (sometimes bloody), wheezing, dyspnea, fatigue, anorexia, weight loss, and a fever.
- Mitral valve prolapse. Most patients with mitral valve prolapse are asymptomatic, but some may experience sharp, stabbing precordial chest pain or precordial ache. The pain can last for seconds or for hours and occasionally mimics the pain of ischemic heart disease. The characteristic sign of mitral prolapse is a midsystolic click followed by a systolic murmur at the apex. Patients may experience cardiac awareness, a migraine headache, dizziness, weakness, episodic severe fatigue, dyspnea, tachycardia, mood swings, and palpitations.
- Myocardial infarction (MI). The chest pain during an MI lasts from 15 minutes to hours. Typically a crushing substernal pain unrelieved by rest or nitroglycerin, it may radiate to the patient’s left arm, jaw, neck, or shoulder blades. Other findings include pallor, clammy skin, dyspnea, diaphoresis, nausea, vomiting, anxiety, restlessness, a feeling of impending doom, hypotension or hypertension, an atrial gallop, murmurs, and crackles.
 GENDER CUE
GENDER CUE
Chest pain in perimenopausal women may be difficult to diagnose because it may be atypical. Fatigue, nausea, dyspnea, and shoulder or neck pain are symptoms more likely to signal an MI in women than in men.
- Pancreatitis. In the acute form, pancreatitis usually causes intense pain in the epigastric area that radiates to the back and worsens when the patient is in a supine position. Nausea, vomiting, a fever, abdominal tenderness and rigidity, diminished bowel sounds, and crackles at the lung bases may also occur. A patient with severe pancreatitis may be extremely restless and have mottled skin, tachycardia, and cold, sweaty extremities. Fulminant pancreatitis causes massive hemorrhage, resulting in shock and coma.
- Peptic ulcer. With a peptic ulcer, sharp and burning pain usually arises in the epigastric region. This pain characteristically arises hours after food intake, commonly during the night. It lasts longer than angina-like pain and is relieved by food or an antacid. Other findings include nausea, vomiting (sometimes with blood), melena, and epigastric tenderness.
- Pericarditis. Pericarditis produces precordial or retrosternal pain aggravated by deep breathing, coughing, position changes, and occasionally swallowing. The pain is commonly sharp or cutting and radiates to the shoulder and neck. Associated signs and symptoms include a pericardial friction rub, a fever, tachycardia, and dyspnea. Pericarditis usually follows a viral illness, but several other causes should be considered.
- Plague (Yersinia pestis). Plague is one of the most virulent bacterial infections and, if untreated, one of the most potentially lethal diseases known. Most cases are sporadic, but the potential for epidemic spread still exists. Clinical forms include bubonic (the most common), septicemic, and pneumonic plagues. The bubonic form is transmitted to a human when bitten by an infected flea. Signs and symptoms include fever, chills, and swollen, inflamed, and tender lymph nodes near the site of the flea bite. Septicemic plague develops as a fulminant illness generally with the bubonic form. The pneumonic form may be contracted from person to person through direct contact via the respiratory system or through biological warfare from aerosolization and inhalation of the organism. The onset is usually sudden with chills, a fever, a headache, and myalgia. Pulmonary signs and symptoms include a productive cough, chest pain, tachypnea, dyspnea, hemoptysis, increasing respiratory distress, and cardiopulmonary insufficiency.
- Pleurisy. The chest pain of pleurisy arises abruptly and reaches maximum intensity within a few hours. The pain is sharp, even knifelike, usually unilateral, and located in the lower and lateral aspects of the chest. Deep breathing, coughing, or thoracic movement characteristically aggravates it. Auscultation over the painful area may reveal decreased breath sounds, inspiratory crackles, and a pleural friction rub. Dyspnea; rapid, shallow breathing; cyanosis; a fever; and fatigue may also occur.
- Pneumonia. Pneumonia produces pleuritic chest pain that increases with deep inspiration and is accompanied by shaking chills and fever. The patient has a dry cough that later becomes productive. Other signs and symptoms include crackles, rhonchi, tachycardia, tachypnea, myalgia, fatigue, a headache, dyspnea, abdominal pain, anorexia, cyanosis, decreased breath sounds, and diaphoresis.
- Pneumothorax. Spontaneous pneumothorax, a life-threatening disorder, causes sudden sharp chest pain that’s severe, typically unilateral, and rarely localized; it increases with chest movement. When the pain is centrally located and radiates to the neck, it may mimic that of an MI. After the pain’s onset, dyspnea and cyanosis progressively worsen. Breath sounds are decreased or absent on the affected side with hyperresonance or tympany, subcutaneous crepitation, and decreased vocal fremitus. Asymmetrical chest expansion, accessory muscle use, a nonproductive cough, tachypnea, tachycardia, anxiety, and restlessness also occur.
- Pulmonary embolism. A pulmonary embolism is a blockage of an artery in the lungs typically caused by a deep vein thrombus that produces chest pain or a choking sensation. Typically, the patient first experiences sudden dyspnea with intense angina-like or pleuritic pain aggravated by deep breathing and thoracic movement. Other findings include tachycardia, tachypnea, a cough (nonproductive or producing blood-tinged sputum), a low-grade fever, restlessness, diaphoresis, crackles, a pleural friction rub, diffuse wheezing, dullness to percussion, signs of circulatory collapse (a weak, rapid pulse; hypotension), paradoxical pulse, signs of cerebral ischemia (transient unconsciousness, coma, seizures), signs of hypoxia (restlessness) and, particularly in the elderly, hemiplegia and other focal neurologic deficits. Less common signs include massive hemoptysis, chest splinting, and leg edema. A patient with a large embolus may have cyanosis and jugular vein distention.
- Q fever. Q fever is a rickettsial disease caused by Coxiella burnetii. The primary source of human infection results from exposure to infected animals. Cattle, sheep, and goats are most likely to carry the organism. Human infection results from exposure to contaminated milk, urine, feces, or other fluids from infected animals. Infection may also result from inhaling contaminated barnyard dust. C. burnetii is highly infectious and is considered a possible airborne agent for biological warfare. Signs and symptoms include a fever, chills, a severe headache, malaise, chest pain, nausea, vomiting, and diarrhea. The fever may last up to 2 weeks. In severe cases, the patient may develop hepatitis or pneumonia.
- Sickle cell crisis. Chest pain associated with sickle cell crisis typically has a bizarre distribution. It may start as a vague pain, commonly located in the back, hands, or feet. As the pain worsens, it becomes generalized or localized to the abdomen or chest, causing severe pleuritic pain. The presence of chest pain and difficulty breathing requires prompt intervention. The patient may also have abdominal distention and rigidity, dyspnea, a fever, and jaundice.
- Thoracic outlet syndrome. Commonly causing paresthesia along the ulnar distribution of the arm, thoracic outlet syndrome can be confused with angina, especially when it affects the left arm. The patient usually experiences angina-like pain after lifting his arms above his head, working with his hands above his shoulders, or lifting a weight. The pain disappears as soon as he lowers his arms. Other signs and symptoms include pale skin and a difference in blood pressure between both arms.
- Tuberculosis (TB). In a patient with TB, pleuritic chest pain and fine crackles occur after coughing. Associated signs and symptoms include night sweats, anorexia, weight loss, a fever, malaise, dyspnea, easy fatigability, a mild to severe productive cough, occasional hemoptysis, dullness to percussion, increased tactile fremitus, and amphoric breath sounds.
- Tularemia. Also known as rabbit fever, tularemia is an infectious disease that’s caused by the gram-negative, non–spore-forming bacterium Francisella tularensis. It’s typically a rural disease found in wild animals, water, and moist soil. It’s transmitted to humans through a bite by an infected insect or tick, handling infected animal carcasses, drinking contaminated water, or inhaling the bacteria. It’s considered a possible airborne agent for biological warfare. Signs and symptoms following inhalation of the organism include the abrupt onset of a fever, chills, a headache, generalized myalgia, a nonproductive cough, dyspnea, pleuritic chest pain, and empyema.
Other Causes
- Chinese restaurant syndrome (CRS). CRS is a benign condition — a reaction to excessive ingestion of monosodium glutamate, a common additive in Chinese foods — that mimics the signs of an acute MI. The patient may complain of retrosternal burning, ache, or pressure; a burning sensation over his arms, legs, and face; a sensation of facial pressure; a headache; shortness of breath; and tachycardia.
- Drugs. The abrupt withdrawal of a beta-adrenergic blocker can cause rebound angina if the patient has coronary heart disease — especially if he has received high doses for a prolonged period.
Special Considerations
As needed, prepare the patient for cardiopulmonary studies, such as an electrocardiogram and a lung scan. Collect a serum sample for cardiac enzyme and electrolyte levels. Explain the purpose and procedure of each diagnostic test to the patient to help alleviate his anxiety. Also, explain the purpose of any prescribed drugs, and make sure that the patient understands the dosage, schedule, and possible adverse effects.
Keep in mind that a patient with chest pain may deny his discomfort, so stress the importance of reporting symptoms to allow adjustment of his treatment.
Patient Counseling
Alert the patient or caregiver to signs and symptoms that require medical attention. Explain the diagnostic tests needed. Provide instructions about any prescribed drugs.
Pediatric Pointers
Even a child old enough to talk may have difficulty describing chest pain, so be alert for nonverbal clues, such as restlessness, facial grimaces, or holding of the painful area. Ask the child to point to the painful area and then to where the pain goes (to find out if it’s radiating). Determine the pain’s severity by asking the parents if the pain interferes with the child’s normal activities and behavior. Remember, a child may complain of chest pain in an attempt to get attention or to avoid attending school.
Geriatric Pointers
Because older patients have a higher risk of developing life- threatening conditions (such as an MI, angina, and aortic dissection), you must carefully evaluate chest pain in these patients.
REFERENCES
Hoffmann, U., Truong, Q. A., Schoenfeld, D. A., Chou, E. T., Woodard, P. K., Nagurney, J. T., … Udelson, J. E.; for the ROMICAT-II Investigators. (2012). Coronary CT angiography versus standard evaluation in acute chest pain. New England Journal of Medicine, 367(4), 299–308.
Miller, C. D., Hwang, W., Hoekstra, J. W., Case, D., Lefebvre, C., & Blumstein, H. (2010). Stress cardiac magnetic resonance imaging with observation unit care reduces cost for patients with emergent chest pain: A randomized trial. Annals of Emergency Medicine, 56(3), 209–219.
Cheyne-Stokes Respirations
The most common pattern of periodic breathing, Cheyne-Stokes respirations are characterized by a waxing and waning period of hyperpnea that alternates with a shorter period of apnea. This pattern can occur normally in patients with heart or lung disease. It usually indicates increased intracranial pressure (ICP) from a deep cerebral or brain stem lesion or a metabolic disturbance in the brain.
Cheyne-Stokes respirations may indicate a major change in the patient’s condition — usually a deterioration. For example, in a patient who has had head trauma or brain surgery, Cheyne-Stokes respirations may signal increasing ICP. Cheyne-Stokes respirations can occur normally in a patient who lives at high altitudes.
Time the periods of hyperpnea and apnea for 3 to 4 minutes to evaluate respirations and to obtain baseline data. Be alert for prolonged periods of apnea. Frequently check the patient’s blood pressure; also check his skin color to detect signs of hypoxemia. Maintain airway patency and administer oxygen as needed. If the patient’s condition worsens, endotracheal intubation is necessary.
 EMERGENCY INTERVENTIONS
EMERGENCY INTERVENTIONS
If you detect Cheyne-Stokes respirations in a patient with a history of head trauma, recent brain surgery, or another brain insult, quickly take his vital signs. Keep his head elevated 30 degrees, and perform a rapid neurologic examination to obtain baseline data. Reevaluate the patient’s neurologic status frequently. If ICP continues to rise, you’ll detect changes in the patient’s level of consciousness (LOC), pupillary reactions, and ability to move his extremities. ICP monitoring is indicated.
History and Physical Examination
If the patient’s condition permits, obtain a brief history. Ask especially about drug use.
Medical Causes
- Heart failure. With left-sided heart failure, Cheyne-Stokes respirations may occur with exertional dyspnea and orthopnea. Related findings include fatigue, weakness, tachycardia, tachypnea, and crackles. The patient may also have a cough, generally nonproductive but occasionally producing clear or blood-tinged sputum.
- Hypertensive encephalopathy. Hypertensive encephalopathy is a life-threatening disorder in which severe hypertension precedes Cheyne-Stokes respirations. The patient’s LOC is decreased, and he may experience vomiting, seizures, severe headaches, papilledema vision disturbances (including transient blindness), or transient paralysis.
- Increased ICP. As ICP rises, Cheyne-Stokes respirations are the first irregular respiratory pattern to occur. It’s preceded by a decreased LOC and accompanied by hypertension, headache, vomiting, impaired or unequal motor movement, and vision disturbances (blurring, diplopia, photophobia, and pupillary changes). In late stages of increased ICP, bradycardia and a widened pulse pressure occur.
- Renal failure. With end-stage chronic renal failure, Cheyne-Stokes respirations may occur in addition to bleeding gums, oral lesions, ammonia breath odor, and marked changes in every body system.
Other Causes
- Drugs. Large doses of an opioid, a hypnotic, or a barbiturate can precipitate Cheyne-Stokes respirations.
Special Considerations
When evaluating Cheyne-Stokes respirations, be careful not to mistake periods of hypoventilation or decreased tidal volume for complete apnea.
Patient Counseling
Teach the patient and a responsible person to recognize the difference between sleep apnea and Cheyne-Stokes respirations. Explain the causes and treatments.
Pediatric Pointers
Cheyne-Stokes respirations rarely occur in children, except during late heart failure.
Geriatric Pointers
Cheyne-Stokes respirations can occur normally in elderly patients during sleep.
REFERENCES
D’Elia, E., Vanoli, E., La Rovere, M. T., Fanfulla, F., Maggioni, A., Casali, V., … Mortara, A. (2012). Adaptive servo ventilation reduces central sleep apnea in chronic heart failure patients: Beneficial effects on autonomic modulation of heart rate. Journal of Cardiovascular Medicine, 14(4), 296–300.
Randerath, W. J., Nothofer, G., Priegnitz, C., Anduleit, N., Treml, M., Kehl, V., Galetke, W. (2012). Long-term auto servo-ventilation or constant positive pressure in heart failure and co-existing central with obstructive sleep apnea. Chest, 143(6), 1833.
Chills[Rigors]
Chills are extreme, involuntary muscle contractions with characteristic paroxysms of violent shivering and teeth chattering. Commonly accompanied by a fever, chills tend to arise suddenly, usually heralding the onset of infection. Certain diseases, such as pneumococcal pneumonia, produce only a single, shaking chill. Other diseases, such as malaria and Hodgkin’s disease (Pel-Ebstein fever), produce intermittent chills with recurring high fever. Still others produce continuous chills for up to 1 hour, precipitating a high fever. (See Why Chills Accompany Fever.)
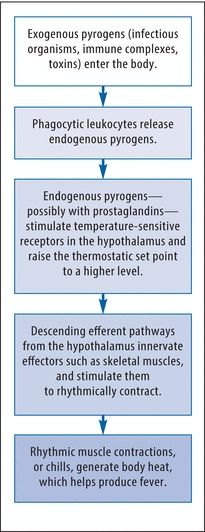
Why Chills Accompany Fever
Fever usually occurs when exogenous pyrogens activate endogenous pyrogens to reset the body’s thermostat to a higher level. At this higher set point, the body feels cold and responds through several compensatory mechanisms, including rhythmic muscle contractions or chills. These muscle contractions generate body heat and help produce fever. This flowchart outlines the events that link chills to fever.
Chills can also result from lymphomas, blood transfusion reactions, and certain drugs. Chills without fever occur as a normal response to exposure to cold. (See Rare Causes of Chills, page 166.)
History and Physical Examination
Ask the patient when the chills began and whether they’re continuous or intermittent. Because fever commonly accompanies or follows chills, take his rectal temperature to obtain a baseline reading. Then, check his temperature often to monitor fluctuations and to determine his temperature curve. Typically, a localized infection produces a sudden onset of shaking chills, sweats, and high fever. A systemic infection produces intermittent chills with recurring episodes of high fever or continuous chills that may last up to 1 hour and precipitate a high fever.
Ask about related signs and symptoms, such as headache, dysuria, diarrhea, confusion, abdominal pain, cough, sore throat, or nausea. Does the patient have any known allergies, an infection, or a recent history of an infectious disorder? Find out which medications he’s taking and whether a drug has improved or worsened his symptoms. Has he received treatment that may predispose him to an infection (such as chemotherapy)? Ask about recent exposure to farm and domestic animals such as guinea pigs, hamsters and dogs, and such birds as pigeons, parrots, and parakeets. Also, ask about recent insect or animal bites, travel to foreign countries, and contact with persons who have an active infection.
Medical Causes
- Acquired immunodeficiency syndrome (AIDS). AIDS is a commonly fatal disease that’s caused by infection with the human immunodeficiency virus transmitted by blood or semen. The patient usually develops lymphadenopathy and may also experience fatigue, anorexia and weight loss, diarrhea, diaphoresis, skin disorders, and signs of upper respiratory tract infection. Opportunistic infections can cause serious disease in the patient with AIDS.
- Anthrax (inhalation). Anthrax is an acute infectious disease that’s caused by the gram-positive, spore-forming bacterium Bacillus anthracis. Although the disease most commonly occurs in wild and domestic grazing animals, such as cattle, sheep, and goats, the spores can live in the soil for many years. The disease can occur in humans exposed to infected animals, tissue from infected animals, or biological warfare. Most natural cases occur in agricultural regions worldwide. Anthrax may occur in a cutaneous, inhalation, or GI form.
Inhalation anthrax is caused by inhalation of aerosolized spores. Initial signs and symptoms are flulike and include a fever, chills, weakness, a cough, and chest pain. The disease generally occurs in two stages with a period of recovery after the initial signs and symptoms. The second stage develops abruptly with rapid deterioration marked by a fever, dyspnea, stridor, and hypotension generally leading to death within 24 hours. Radiologic findings include mediastinitis and symmetric mediastinal widening.
- Cholangitis. Charcot’s triad — chills with spiking fever, right upper quadrant abdominal pain, and jaundice — characterizes a sudden obstruction of the common bile duct. The patient may have associated pruritus, weakness, and fatigue.
- Gram-negative bacteremia. Gram-negative bacteremia causes sudden chills and a fever, nausea, vomiting, diarrhea, and prostration.
- Hemolytic anemia. With acute hemolytic anemia, fulminating chills occur with a fever and abdominal pain. The patient rapidly develops jaundice and hepatomegaly; he may develop splenomegaly.
- Hepatic abscess. Hepatic abscess usually arises abruptly, with chills, a fever, nausea, vomiting, diarrhea, anorexia, and severe upper abdominal tenderness and pain that may radiate to the right shoulder.
- Infective endocarditis. Infective endocarditis produces the abrupt onset of intermittent, shaking chills with a fever. Petechiae commonly develop. The patient may also have Janeway lesions on his hands and feet and Osler’s nodes on his palms and soles. Associated findings include a murmur, hematuria, eye hemorrhage, Roth’s spots, and signs of cardiac failure (dyspnea, peripheral edema).
- Influenza. Initially, influenza causes an abrupt onset of chills, a high fever, malaise, a headache, myalgia, and a nonproductive cough. Some patients may also suddenly develop rhinitis, rhinorrhea, laryngitis, conjunctivitis, hoarseness, and a sore throat. Chills generally subside after the first few days, but an intermittent fever, weakness, and a cough may persist for up to 1 week.
- Kawasaki disease. Kawasaki disease, an acute febrile illness of unknown etiology, primarily affects children younger than 5 years of age, predominantly boys. Chills result from a high spiking fever that usually lasts 5 days or more. Accompanying symptoms include irritability, red eyes, bright red cracked lips, a strawberry tongue, swollen hands and feet, peeling skin on the fingertips and toes, and cervical lymphadenopathy. More severe complications include inflammation in the walls of arteries throughout the body, including the coronary arteries. Standard treatment with intravenous immunoglobulin and aspirin substantially decreases the development of these coronary artery abnormalities, and most children recover without serious problems. Although Kawasaki disease occurs worldwide, with the highest incidence in Japan, it is a leading cause of acquired heart disease in children in the United States.
- Legionnaires’ disease. Within 12 to 48 hours after the onset of Legionnaires’ disease, the patient suddenly develops chills and a high fever. Prodromal signs and symptoms characteristically include malaise, a headache, and possibly diarrhea, anorexia, diffuse myalgia, and general weakness. An initially nonproductive cough progresses to a productive cough with mucoid or mucopurulent sputum and possibly hemoptysis. The patient usually also develops nausea and vomiting, confusion, mild temporary amnesia, pleuritic chest pain, dyspnea, tachypnea, crackles, tachycardia, and flushed and mildly diaphoretic skin.
Rare Causes of Chills
Chills can result from disorders that rarely occur in the United States, but may be fairly common worldwide. Remember to ask about recent foreign travel when you obtain a patient’s history. Keep in mind this is only a partial list of rare disorders that produce chills.
- Brucellosis (undulant fever)
- Dengue fever (breakbone fever)
- Epidemic typhus (louse-borne typhus)
- Leptospirosis
- Lymphocytic choriomeningitis
- Monkey pox
- Plague
- Pulmonary tularemia
- Rat bite fever
- Relapsing fever
- Malaria. The paroxysmal cycle of malaria begins with a period of chills lasting 1 to 2 hours. This is followed by a high fever lasting 3 to 4 hours and then 2 to 4 hours of profuse diaphoresis. Paroxysms occur every 48 to 72 hours when caused by Plasmodium malariae and every 40 to 42 hours when caused by P. vivax or P. ovale. With benign malaria, the paroxysms may be interspersed with periods of well-being. The patient also has a headache, muscle pain and, possibly, hepatosplenomegaly.
- Monkey pox. Primarily a disease found in monkeys in central and western Africa, the monkey pox virus infrequently attacks humans. Several humans contracted the virus from infected prairie dogs in the United States in 2003. Initial symptoms of patients infected with monkey pox are chills resulting from a fever. Symptoms are similar to, but milder than, smallpox. Other common findings of this rare disease are sore throat, swollen lymph nodes, cough, shortness of breath, headache, muscle aches, backache, a general feeling of discomfort and exhaustion, and the development of a rash. There is no treatment for monkey pox infections. In certain cases, the smallpox vaccine is used to protect individuals against monkey pox or to lessen the severity of the disease.
- Pelvic inflammatory disease. Pelvic inflammatory disease causes chills and fever with, typically, lower abdominal pain and tenderness; profuse, purulent vaginal discharge; or abnormal menstrual bleeding. The patient may also develop nausea and vomiting, an abdominal mass, and dysuria.
- Plague (Yersinia pestis). Plague is one of the most virulent bacterial infections and, if untreated, one of the most potentially lethal diseases known. Most cases are sporadic, but the potential for epidemic spread still exists. Clinical forms include bubonic (the most common), septicemic, and pneumonic plagues. The bubonic form is transmitted to a human when bitten by an infected flea. Signs and symptoms include a fever, chills, and swollen, inflamed, and tender lymph nodes near the site of the flea bite. Septicemic plague develops as a fulminant illness generally with the bubonic form. The pneumonic form may be contracted from person to person through direct contact via the respiratory system or through biological warfare from aerosolization and inhalation of the organism. The onset is usually sudden with chills, a fever, headache, and myalgia. Pulmonary signs and symptoms include a productive cough, chest pain, tachypnea, dyspnea, hemoptysis, increasing respiratory distress, and cardiopulmonary insufficiency.
- Pneumonia. A single shaking chill usually heralds the sudden onset of pneumococcal pneumonia; other pneumonias characteristically cause intermittent chills. With any type of pneumonia, related findings may include a fever, a productive cough with bloody sputum, pleuritic chest pain, dyspnea, tachypnea, and tachycardia. The patient may be cyanotic and diaphoretic, with bronchial breath sounds and crackles, rhonchi, increased tactile fremitus, and grunting respirations. He may also experience achiness, anorexia, fatigue, and a headache.
- Puerperal or postabortal sepsis. Chills and a high fever occur as early as 6 hours or as late as 10 days postpartum or postabortion. The patient may also have a purulent vaginal discharge, an enlarged and tender uterus, abdominal pain, backache and, possibly, nausea, vomiting, and diarrhea.
- Pyelonephritis. With acute pyelonephritis, the patient develops chills, a high fever, and possibly nausea and vomiting over several hours to days. He generally also has anorexia, fatigue, myalgia, flank pain, costovertebral angle (CVA) tenderness, hematuria or cloudy urine, and urinary frequency, urgency, and burning.
- Q fever. Q fever is a rickettsial disease caused by Coxiella burnetii. The primary source of human infection results from exposure to infected animals. Cattle, sheep, and goats are most likely to carry the organism. Human infection results from exposure to contaminated milk, urine, feces, or other fluids from infected animals. Infection may also result from inhalation of contaminated barnyard dust. C. burnetii is highly infectious and is considered a possible airborne agent for biological warfare. Signs and symptoms include a fever, chills, a severe headache, malaise, chest pain, nausea, vomiting, and diarrhea. The fever may last up to 2 weeks. In severe cases, the patient may develop hepatitis or pneumonia.
- Renal abscess. Renal abscess initially produces sudden chills and a fever. Later effects include flank pain, CVA tenderness, abdominal muscle spasm, and transient hematuria.
- Rocky Mountain spotted fever. Rocky Mountain spotted fever begins with a sudden onset of chills, a fever, malaise, an excruciating headache, and muscle, bone, and joint pain. Typically, the patient’s tongue is covered with a thick white coating that gradually turns brown. After 2 to 6 days of fever and occasional chills, a macular or maculopapular rash appears on the hands and feet and then becomes generalized; after a few days, the rash becomes petechial.
- Septic arthritis. Chills and fever accompany the characteristic red, swollen, and painful joints caused by septic arthritis.
- Septic shock. Initially, septic shock produces chills, a fever, and, possibly, nausea, vomiting, and diarrhea. The patient’s skin is typically flushed, warm, and dry; his blood pressure is normal or slightly low; and he has tachycardia and tachypnea. As septic shock progresses, the patient’s arms and legs become cool and cyanotic, and he develops oliguria, thirst, anxiety, restlessness, confusion, and hypotension. Later, his skin becomes cold and clammy and his pulse, rapid and thready. He further develops severe hypotension, persistent oliguria or anuria, signs of respiratory failure, and coma.
- Sinusitis. With acute sinusitis, chills occur along with a fever, a headache, and pain, tenderness, and swelling over the affected sinuses. Maxillary sinusitis produces pain over the cheeks and upper teeth; ethmoid sinusitis, pain over the eyes; frontal sinusitis, pain over the eyebrows; and sphenoid sinusitis, pain behind the eyes. The primary indicator of sinusitis is nasal discharge, which is commonly bloody for 24 to 48 hours before it gradually becomes purulent.
- Snake bite. Most pit viper bites that result in envenomization cause chills, typically with a fever. Other systemic signs and symptoms include sweating, weakness, dizziness, fainting, hypotension, nausea, vomiting, diarrhea, and thirst. The area around the snake bite may be marked by immediate swelling and tenderness, pain, ecchymoses, petechiae, blebs, bloody discharge, and local necrosis. The patient may have difficulty speaking, blurred vision, and paralysis. He may also show bleeding tendencies and signs of respiratory distress and shock.
- Tularemia. Also known as rabbit fever, tularemia is an infectious disease that’s caused by the gram-negative, non–spore-forming bacterium Francisella tularensis. It’s typically a rural disease found in wild animals, water, and moist soil. It’s transmitted to humans through the bite of an infected insect or tick, handling infected animal carcasses, drinking contaminated water, or inhaling the bacteria. It’s considered a possible airborne agent for biological warfare. Signs and symptoms following inhalation of the organism include the abrupt onset of a fever, chills, a headache, generalized myalgia, a nonproductive cough, dyspnea, pleuritic chest pain, and empyema.
- Typhus. Typhus is a rickettsial disease transmitted to humans by fleas, mites, or body lice. Initial signs and symptoms include a headache, myalgia, arthralgia, and malaise followed by an abrupt onset of chills, a fever, nausea, and vomiting. A maculopapular rash may be present in some cases.
- Violin spider bite. The violin spider bite produces chills, a fever, malaise, weakness, nausea, vomiting, and joint pain within 24 to 48 hours. The patient may also develop a rash and delirium.
Other Causes
- Drugs. Amphotericin B is a drug associated with chills. Phenytoin is also a common cause of drug-induced fever that can produce chills. I.V. bleomycin and intermittent administration of an oral antipyretic can also cause chills.
- I.V. therapy. Infection at the I.V. insertion site (superficial phlebitis) can cause chills, high fever, and local redness, warmth, induration, and tenderness.
- Transfusion reaction. A hemolytic reaction may cause chills during the transfusion or immediately afterward. A nonhemolytic febrile reaction may also cause chills.
Special Considerations
Check the patient’s vital signs often, especially if his chills result from a known or suspected infection. Be alert for signs of progressive septic shock, such as hypotension, tachycardia, and tachypnea. If appropriate, obtain samples of blood, sputum, wound drainage, or urine for culture to determine the causative organism. Give the appropriate antibiotic. Radiographic studies may be required.
Because chills are an involuntary response to an increased body temperature set by the hypothalamic thermostat, blankets won’t stop a patient’s chills or shivering. Despite this, keep his room temperature as even as possible. Provide adequate hydration and nutrients, and give an antipyretic to help control a fever. The irregular use of an antipyretic can trigger compensatory chills.
Patient Counseling
Explain to the patient the following: the importance of documenting temperature to reveal patterns, the necessary treatment and antibiotics, the signs and symptoms of a worsening condition, and when to seek medical attention.
Pediatric Pointers
Infants don’t get chills because they have poorly developed shivering mechanisms. In addition, most classic febrile childhood infections, such as measles and mumps, don’t typically produce chills. However, older children and teenagers may have chills with mycoplasma pneumonia and acute pyogenic osteomyelitis.
Geriatric Pointers
Chills in an elderly patient usually indicate an underlying infection, such as a urinary tract infection, pneumonia (commonly associated with aspiration of gastric contents), diverticulitis, or skin breakdown in pressure areas. Also, consider an ischemic bowel in an elderly patient who comes into your facility with a fever, chills, and abdominal pain.
REFERENCES
Tang, Y. W., Himmelfarb, E., Wills, M., & Stratton, C. W. (2010). Characterization of three staphylococcus aureus isolates from a 17-year-old female who died of tampon-related toxic shock syndrome. Journal of Clinical Microbiology. 48(5), 1974–1977.
Zaki, S. A., Shanbag, P., Chavan, V., & Shenoy, P. (2010). Staphylococcal toxic shock syndrome presenting as acute respiratory distress and cor pulmonale. Annals of Tropical Paediatrics. 30(1), 77–81.
Chvostek’s Sign
Chvostek’s sign is an abnormal spasm of the facial muscles elicited by lightly tapping the patient’s facial nerve near his lower jaw. (See Eliciting Chvostek’s Sign.) This sign usually suggests hypocalcemia, but can occur normally in about 25% of cases. Typically, it precedes other signs of hypocalcemia and persists until the onset of tetany. It can’t be elicited during tetany because of strong muscle contractions.
Normally, eliciting Chvostek’s sign is attempted only in patients with suspected hypocalcemic disorders. However, because the parathyroid gland regulates calcium balance, Chvostek’s sign may also be tested in patients before neck surgery to obtain a baseline.
 EMERGENCY INTERVENTIONS
EMERGENCY INTERVENTIONS
Test for Trousseau’s sign, a reliable indicator of hypocalcemia. Closely monitor the patient for signs of tetany, such as carpopedal spasms or circumoral and extremity paresthesia.
Be prepared to act rapidly if a seizure occurs. Perform an electrocardiogram to check for changes associated with hypocalcemia that can predispose the patient to arrhythmias. Place the patient on a cardiac monitor.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


