• Most common in head and neck region (up to 80% of cases)
• Prognosis usually excellent, most cases cured by excision
• More aggressive subtypes, including infiltrative, micronodular, desmoplastic, and basosquamous, have higher rate of recurrence and low risk of metastasis
• Treated by complete excision or electrodesiccation and curettage
Microscopic
• Proliferation of nodules, nests, and cords of basaloid cells with peripheral palisading, stromal retraction artifact, and mucinous material
• Numerous mitotic and apoptotic figures typically present
• Cells show enlarged hyperchromatic nuclei with inconspicuous nucleoli and scant amounts of cytoplasm
• Superficial multicentric type: Superficial nests attached to epidermis separated by areas of uninvolved epidermis
• Micronodular type: Predominantly dermal-based infiltrative proliferation of small nests
• Infiltrative type: Small cords and nests, often deeply invasive
• Desmoplastic/sclerosing/morpheaform type: Infiltrative strands and nests associated with dense sclerotic stroma
Top Differential Diagnoses
• Squamous cell carcinoma
• Actinic keratosis (on superficial shave biopsy)
• Follicular neoplasms (trichoepithelioma and trichoblastoma)
• Merkel cell carcinoma
Clinical Photograph of Basal Cell Carcinoma Clinical photograph of a large facial basal cell carcinoma (BCC) shows areas of ulceration and granulation-like tissue surrounded by a raised border . (Courtesy S. Yashar, MD.)
Basal Cell Carcinoma at Low Magnification Low magnification shows a large nodular- and micronodular-type BCC with diffuse overlying ulceration and dense serum crust containing degenerating neutrophils.
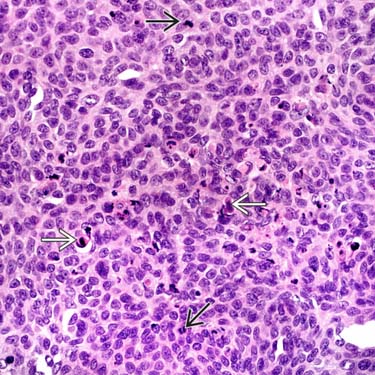
Basal Cell Carcinoma at High Magnification High magnification of a nodular BCC shows a sheet-like proliferation of atypical basaloid cells with high nuclear:cytoplasmic ratios and numerous apoptotic and mitotic figures .
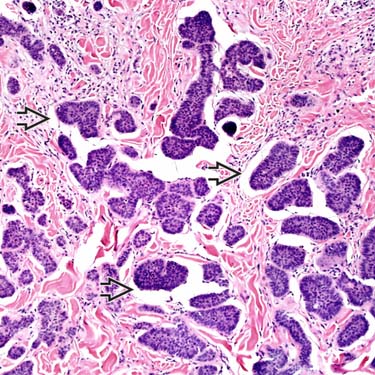
Basal Cell Carcinoma: Micronodular Type Histologic section of a micronodular-type BCC shows a proliferation of small, infiltrative nests of basaloid cells with a prominent retraction artifact in a somewhat sclerotic-appearing stroma.
TERMINOLOGY
Abbreviations
• Basal cell carcinoma (BCC)
Synonyms
• Basal cell epithelioma (BCE)
• Trichoblastic carcinoma (not well accepted and should be discouraged)
Definitions
• Low-grade malignancy of basaloid-appearing keratinocytes
ETIOLOGY/PATHOGENESIS
Multifactorial
• Related to sun exposure (vast majority of cases)
Some cases may also be associated with radiation, immunosuppression (organ transplantation), burn scars
– These cases tend to be more aggressive
• May actually be derived from follicular stem cells (hence, rationale for term trichoblastic carcinoma)
Genetics
• Rare cases are associated with genetic syndromes including nevoid BCC (Gorlin) syndrome, xeroderma pigmentosum, Basex syndrome, Rombo syndrome, and McKusick syndrome
Extremely common: Most common cancer overall in humans when skin cancers are included
– Accounts for 70% of primary cutaneous malignancies
• Age
Typically older adults; few cases in young adults
– If in child, should consider genetic syndrome
• Sex
Slightly greater incidence in male patients
• Ethnicity
Caucasian/light-skinned individuals
Rare in individuals with darker skin types
Site
• Most common in head and neck region (up to 80% of cases)
~ 15% occur on trunk and shoulders
Very rare cases involve lips, breast, axillae, groin, inguinal region, and genitalia
Presentation
• Typically papular, plaque-like, or nodular lesion
Often present as pearly, translucent papule with telangiectasia
Larger lesions often ulcerated with bleeding &/or overlying crusting
Minority of cases are pigmented, more often in Asians and Africans
Treatment
• Surgical approaches
Complete excision or electrodesiccation and curettage
Mohs micrographic surgery often used in facial cases
Prognosis
• Usually excellent, cured by local excision
• More aggressive subtypes, including micronodular, infiltrative, desmoplastic, and basosquamous, have higher rate of recurrence and increased (but still very low) risk of metastasis
Overall risk of metastasis estimated at 0.05%
MACROSCOPIC
Size
• Variable, small (few mm) to large (several cm)
MICROSCOPIC
Histologic Features
• Tumor is composed of nodules, nests, &/or infiltrative cords
Overlying ulceration and serum crusting often present in large tumors
• Proliferation of small basaloid cells with peripheral palisading
• Stromal retraction artifact
Between tumor cells and stroma
• Mucinous material often is present in stroma
• Numerous mitotic and apoptotic figures in most cases
• Cells show enlarged, hyperchromatic-staining nuclei with inconspicuous or small nucleoli and scant eosinophilic cytoplasm
Variants
• Superficial multicentric: Superficial nests attached to epidermis separated by areas of uninvolved epidermis
Only gold members can continue reading. Log In or Register to continue

 . (Courtesy S. Yashar, MD.)
. (Courtesy S. Yashar, MD.)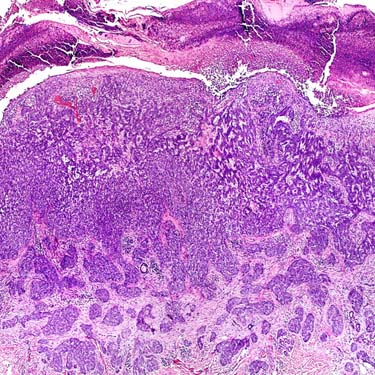
 and mitotic figures
and mitotic figures  .
.
 in a somewhat sclerotic-appearing stroma.
in a somewhat sclerotic-appearing stroma.



















