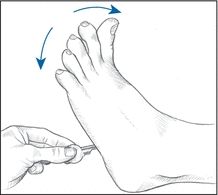
EXAMINATION TIP How to Elicit Babinski’s Reflex
To elicit Babinski’s reflex, stroke the lateral aspect of the sole of the patient’s foot with your thumbnail or another moderately sharp object. Normally, this elicits flexion of all toes (a negative Babinski’s reflex), as shown below in the left illustration. With a positive Babinski’s reflex, the great toe dorsiflexes and the other toes fan out, as shown in the right illustration.
NORMAL TOE FLEXION
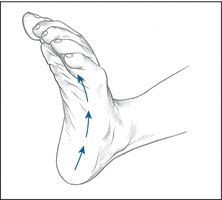
POSITIVE BABINSKI’S REFLEX
- Head trauma. Unilateral or bilateral Babinski’s reflex may occur as the result of primary corticospinal damage or secondary injury associated with increased intracranial pressure. Hyperactive DTRs and spasticity commonly occur with Babinski’s reflex. The patient may also have weakness and incoordination. Other signs and symptoms vary with the type of head trauma and include headache, vomiting, behavior changes, altered vital signs, and decreased LOC with abnormal pupillary size and response to light.
- Hepatic encephalopathy. Babinski’s reflex occurs late in hepatic encephalopathy when the patient slips into a coma. It’s accompanied by hyperactive DTRs and fetor hepaticus.
- Meningitis. With meningitis, bilateral Babinski’s reflex commonly follows fever, chills, and malaise and is accompanied by nausea and vomiting. As meningitis progresses, it also causes decreased LOC, nuchal rigidity, positive Brudzinski’s and Kernig’s signs, hyperactive DTRs, and opisthotonos. Associated signs and symptoms include irritability, photophobia, diplopia, delirium, and deep stupor that may progress to coma.
- Rabies. Bilateral Babinski’s reflex — possibly elicited by nonspecific noxious stimuli alone — appears in the excitation phase of rabies. This phase occurs 2 to 10 days after the onset of prodromal signs and symptoms, such as fever, malaise, and irritability (which occur 30 to 40 days after a bite from an infected animal). Rabies is characterized by marked restlessness and extremely painful pharyngeal muscle spasms. Difficulty swallowing causes excessive drooling and hydrophobia in about 50% of affected patients. Seizures and hyperactive DTRs may also occur.
- Spinal cord injury. With acute injury, spinal shock temporarily erases all reflexes. As shock resolves, Babinski’s reflex occurs — unilaterally when injury affects only one side of the spinal cord (Brown-Séquard syndrome) and bilaterally when injury affects both sides. Rather than signaling the return of neurologic function, this reflex confirms corticospinal damage. It’s accompanied by hyperactive DTRs, spasticity, and variable or total loss of pain and temperature sensation, proprioception, and motor function. Horner’s syndrome, marked by unilateral ptosis, pupillary constriction, and facial anhidrosis, may occur with lower cervical cord injury.
- Spinal cord tumor. With spinal cord tumor, bilateral Babinski’s reflex occurs with variable loss of pain and temperature sensation, proprioception, and motor function. Spasticity, hyperactive DTRs, absent abdominal reflexes, and incontinence are also characteristic. Diffuse pain may occur at the level of the tumor.
- Spinal paralytic poliomyelitis. Unilateral or bilateral Babinski’s reflex occurs 5 to 7 days after the onset of fever. It’s accompanied by progressive weakness, paresthesia, muscle tenderness, spasticity, irritability and, later, atrophy. Resistance to neck flexion is characteristic, as are Hoyne’s, Kernig’s, and Brudzinski’s signs.
- Spinal tuberculosis. Spinal tuberculosis may produce bilateral Babinski’s reflex accompanied by variable loss of pain and temperature sensation, proprioception, and motor function. It also causes spasticity, hyperactive DTRs, bladder incontinence, and absent abdominal reflexes.
- Stroke. Babinski’s reflex varies with the site of the stroke. If it involves the cerebrum, it produces unilateral Babinski’s reflex accompanied by hemiplegia or hemiparesis, unilateral hyperactive DTRs, hemianopsia, and aphasia. If it involves the brain stem, it produces bilateral Babinski’s reflex accompanied by bilateral weakness or paralysis, bilateral hyperactive DTRs, cranial nerve dysfunction, incoordination, and an unsteady gait. Generalized signs and symptoms of stroke include headache, vomiting, fever, disorientation, nuchal rigidity, seizures, and coma.
- Syringomyelia. With syringomyelia, bilateral Babinski’s reflex occurs with muscle atrophy and weakness that may progress to paralysis. It’s accompanied by spasticity, ataxia and, occasionally, deep pain. DTRs may be hypoactive or hyperactive. Cranial nerve dysfunction, such as dysphagia and dysarthria, commonly appears late in the disorder.
Special Considerations
Babinski’s reflex usually occurs with incoordination, weakness, and spasticity, all of which increase the patient’s risk of injury. To prevent injury, assist the patient with activity and keep his environment free from obstructions.
Diagnostic tests may include a computed tomography scan or magnetic resonance imaging of the brain or spine, angiography or myelography and, possibly, a lumbar puncture to clarify or confirm the cause of Babinski’s reflex. Prepare the patient as necessary.
Patient Counseling
Caution the patient about the need to call for assistance when getting out of bed and discuss ways to maintain a safe environment. Instruct the patient in the use of adaptive devices.
Pediatric Pointers
Babinski’s reflex occurs normally in infants ages 18 to 24 months, reflecting immaturity of the corticospinal tract. After age 2, Babinski’s reflex is pathologic and may result from hydrocephalus or any of the causes more commonly seen in adults.
REFERENCES
Caranci, F., Briganti, F., Cirillo, L., Leonardi, M., & Muto, M. (2013). Epidemiology and genetics of intracranial aneurysms. European Journal of Radiology, 82, 1598–1605.
Hetts, S. W., English, J. D., Dowd, C. F., Higashida, R. T., Scanlon, J. T., & Halbach, V. V. (2011). Pediatric intracranial aneurysms: New and enlarging aneurysms after index aneurysm treatment or observation. American Journal of Neuroradiology, 32, 2017–2022.
Back Pain
Back pain affects an estimated 80% of the population; in fact, it’s the second leading reason — after the common cold — for lost time from work. Although this symptom may herald a spondylogenic disorder, it may also result from a genitourinary, GI, cardiovascular, or neoplastic disorder. Postural imbalance associated with pregnancy may also cause back pain.
The onset, location, and distribution of pain and its response to activity and rest provide important clues about the cause. Pain may be acute or chronic, constant or intermittent. It may remain localized in the back, radiate along the spine or down one or both legs, or be widespread. Pain may be exacerbated by activity — usually bending, stooping, lifting, or exercising — and alleviated by rest, or it may be unaffected by either.
Intrinsic back pain results from muscle spasm, nerve root irritation, fracture, or a combination of these mechanisms. It usually occurs in the lower back, or lumbosacral area. Back pain may also be referred from the abdomen or flank, possibly signaling a life-threatening perforated ulcer, acute pancreatitis, or a dissecting abdominal aortic aneurysm.
 EMERGENCY INTERVENTIONS
EMERGENCY INTERVENTIONS
If the patient reports acute, severe back pain, quickly take his vital signs and then perform a rapid evaluation to rule out life-threatening causes. Ask him when the pain began. Can he relate it to any causes? For example, did the pain occur after eating? After falling on the ice? Have the patient describe the pain. Is it burning, stabbing, throbbing, or aching? Is it constant or intermittent? Does it radiate to the buttocks, legs, or toes? Does he have leg weakness or footdrop? Does the pain seem to originate in the abdomen and radiate to the back? Has he had a pain like this before? What makes it better or worse? Is it affected by activity or rest? Is it worse in the morning or evening? Does it wake him up? Typically, visceral-referred back pain is unaffected by activity and rest. In contrast, spondylogenic-referred back pain worsens with activity and improves with rest. Pain of neoplastic origin is usually relieved by walking and worsens at night.
If the patient describes deep lumbar pain unaffected by activity, palpate for a pulsating epigastric mass. If this sign is present, suspect a dissecting abdominal aortic aneurysm. Withhold food and fluid in anticipation of emergency surgery. Prepare for I.V. fluid replacement and oxygen administration. Monitor the patient’s vital signs and peripheral pulses closely.
If the patient describes severe epigastric pain that radiates through the abdomen to the back, assess him for absent bowel sounds and for abdominal rigidity and tenderness. If these occur, suspect a perforated ulcer or acute pancreatitis. Start an I.V. for fluids and drugs, administer oxygen, and insert a nasogastric tube while withholding food.
History and Physical Examination
If life-threatening causes of back pain are ruled out, continue with a complete history and physical examination. Be aware of the patient’s expressions of pain as you do so. Obtain a medical history, including past injuries and illnesses, and a family history. Ask about diet and alcohol intake. Also, take a drug history, including past and present prescriptions and over-the-counter drugs.
Next, perform a thorough physical examination. Observe skin color, especially in the patient’s legs, and palpate skin temperature. Palpate femoral, popliteal, posterior tibial, and pedal pulses. Ask about unusual sensations in the legs, such as numbness and tingling. Observe the patient’s posture if pain doesn’t prohibit standing. Does he stand erect or tend to lean toward one side? Observe the level of the shoulders and pelvis and the curvature of the back. Ask the patient to bend forward, backward, and from side to side while you palpate for paravertebral muscle spasms. Note rotation of the spine on the trunk. Palpate the dorsolumbar spine for point tenderness. Then, ask the patient to walk — first on his heels and then on his toes — protect him from falling as he does so. Weakness may reflect a muscular disorder or spinal nerve root irritation. Place the patient in a sitting position to evaluate and compare patellar tendon (knee), Achilles tendon, and Babinski’s reflexes. Evaluate the strength of the extensor hallucis longus by asking the patient to hold up his big toe against resistance. Measure leg length and hamstring and quadriceps muscles bilaterally. Note a difference of more than ⅜” (1 cm) in muscle size, especially in the calf.
To reproduce leg and back pain, position the patient in a supine position on the examining table. Grasp his heel and slowly lift his leg. If he feels pain, note its exact location and the angle between the table and his leg when it occurs. Repeat this maneuver with the opposite leg. Pain along the sciatic nerve may indicate disk herniation or sciatica. Also, note the range of motion of the hip and knee.
Palpate the flanks and percuss with the fingertips or perform fist percussion to elicit costovertebral angle tenderness.
Medical Causes
- Abdominal aortic aneurysm (dissecting). Life-threatening dissection of this aneurysm may initially cause low back pain or dull abdominal pain. More commonly, it produces constant upper abdominal pain. A pulsating abdominal mass may be palpated in the epigastrium; after rupture, however, it no longer pulses. Aneurysmal dissection can also cause mottled skin below the waist, absent femoral and pedal pulses, lower blood pressure in the legs than in the arms, mild to moderate tenderness with guarding, and abdominal rigidity. Signs of shock (such as cool, clammy skin) appear if blood loss is significant.
- Ankylosing spondylitis. Ankylosing spondylitis is a chronic, progressive disorder that causes sacroiliac pain, which radiates up the spine and is aggravated by lateral pressure on the pelvis. The pain is usually most severe in the morning or after a period of inactivity and isn’t relieved by rest. Abnormal rigidity of the lumbar spine with forward flexion is also characteristic. This disorder can cause local tenderness, fatigue, fever, anorexia, weight loss, and occasional iritis.
- Appendicitis. Appendicitis is a life-threatening disorder in which a vague and dull discomfort in the epigastric or umbilical region migrates to McBurney’s point in the right lower quadrant. With retrocecal appendicitis, pain may also radiate to the back. The shift in pain is preceded by anorexia and nausea and is accompanied by fever, occasional vomiting, abdominal tenderness (especially over McBurney’s point), and rebound tenderness. Some patients also have painful, urgent urination.
- Cholecystitis. Cholecystitis produces severe pain in the right upper quadrant of the abdomen that may radiate to the right shoulder, chest, or back. The pain may arise suddenly or may increase gradually over several hours, and patients usually have a history of similar pain after a high-fat meal. Accompanying signs and symptoms include anorexia, fever, nausea, vomiting, right upper quadrant tenderness, abdominal rigidity, pallor, and sweating.
- Chordoma. A slow-developing malignant tumor, chordoma causes persistent pain in the lower back, sacrum, and coccyx. As the tumor expands, pain may be accompanied by constipation and bowel or bladder incontinence.
- Endometriosis. Endometriosis causes deep sacral pain and severe, cramping pain in the lower abdomen. The pain worsens just before or during menstruation and may be aggravated by defecation. It’s accompanied by constipation, abdominal tenderness, dysmenorrhea, and dyspareunia.
- Intervertebral disk rupture. Intervertebral disk rupture produces gradual or sudden low back pain with or without leg pain (sciatica). It rarely produces leg pain alone. Pain usually begins in the back and radiates to the buttocks and leg. The pain is exacerbated by activity, coughing, and sneezing and is eased by rest. It’s accompanied by paresthesia (most commonly, numbness or tingling in the lower leg and foot), paravertebral muscle spasm, and decreased reflexes on the affected side. This disorder also affects posture and gait. The patient’s spine is slightly flexed and he leans toward the painful side. He walks slowly and rises from a sitting to a standing position with extreme difficulty.
- Lumbosacral sprain. Lumbosacral sprain causes aching, localized pain, and tenderness associated with muscle spasm on lateral motion. The recumbent patient typically flexes his knees and hips to help ease pain. Flexion of the spine intensifies pain, whereas rest helps relieve it. The pain worsens with movement and is relieved by rest.
- Metastatic tumors. Metastatic tumors commonly spread to the spine, causing low back pain in at least 25% of patients. Typically, the pain begins abruptly, is accompanied by cramping muscular pain (usually worse at night), and isn’t relieved by rest.
- Myeloma. Back pain caused by myeloma, a primary malignant tumor, usually begins abruptly and worsens with exercise. It may be accompanied by arthritic signs and symptoms, such as achiness, joint swelling, and tenderness. Other signs and symptoms include fever, malaise, peripheral paresthesia, and weight loss.
- Pancreatitis (acute). Pancreatitis is a life-threatening disorder that usually produces fulminating, continuous upper abdominal pain that may radiate to both flanks and to the back. To relieve this pain, the patient may bend forward, draw his knees to his chest, or move restlessly about.
Early associated signs and symptoms include abdominal tenderness, nausea, vomiting, fever, pallor, tachycardia and, in some patients, abdominal guarding, rigidity, rebound tenderness, and hypoactive bowel sounds. A late sign may be jaundice. Occurring as inflammation subsides, Turner’s sign (ecchymosis of the abdomen or flank) or Cullen’s sign (bluish discoloration of skin around the umbilicus and in both flanks) signals hemorrhagic pancreatitis.
- Perforated ulcer. In some patients, perforation of a duodenal or gastric ulcer causes sudden, prostrating epigastric pain that may radiate throughout the abdomen and to the back. This life-threatening disorder also causes boardlike abdominal rigidity; tenderness with guarding; generalized rebound tenderness; the absence of bowel sounds; and grunting, shallow respirations. Associated signs include fever, tachycardia, and hypotension.
- Prostate cancer. Chronic aching back pain may be the only symptom of prostate cancer. This disorder may also produce hematuria and decrease the urine stream.
- Pyelonephritis (acute). Pyelonephritis produces progressive flank and lower abdominal pain accompanied by back pain or tenderness (especially over the costovertebral angle). Other signs and symptoms include high fever and chills, nausea and vomiting, flank and abdominal tenderness, and urinary frequency and urgency.
- Renal calculi. The colicky pain of renal calculi usually results from irritation of the ureteral lining, which increases the frequency and force of peristaltic contractions. The pain travels from the costovertebral angle to the flank, suprapubic region, and external genitalia. Its intensity varies but may become excruciating if calculi travel down a ureter. If calculi are in the renal pelvis and calyces, dull and constant flank pain may occur. Renal calculi also cause nausea, vomiting, urinary urgency (if a calculus lodges near the bladder), hematuria, and agitation due to pain. Pain resolves or significantly decreases after calculi move to the bladder. Encourage the patient to recover the calculi for analysis.
- Rift Valley fever. Rift Valley fever is a viral disease generally found in Africa, but in 2000, outbreaks occurred in Saudi Arabia and Yemen. It’s transmitted to humans from the bite of an infected mosquito or from exposure to infected animals. Rift Valley fever may present as several different clinical syndromes. Typical signs and symptoms include fever, myalgia, weakness, dizziness, and back pain. A small percentage of patients may develop encephalitis or may progress to hemorrhagic fever that can lead to shock and hemorrhage. Inflammation of the retina may result in some permanent vision loss.
- Sacroiliac strain. Sacroiliac strain causes sacroiliac pain that may radiate to the buttock, hip, and lateral aspect of the thigh. The pain is aggravated by weight bearing on the affected extremity and by abduction with resistance of the leg. Associated signs and symptoms include tenderness of the symphysis pubis and a limp or gluteus medius or abductor lurch.
- Smallpox (variola major). Worldwide eradication of smallpox was achieved in 1977; the United States and Russia have the only known storage sites of the virus. The virus is considered a potential agent for biological warfare. Initial signs and symptoms include high fever, malaise, prostration, severe headache, backache, and abdominal pain. A maculopapular rash develops on the mucosa of the mouth, pharynx, face, and forearms and then spreads to the trunk and legs. Within 2 days, the rash becomes vesicular and later pustular. The lesions develop at the same time, appear identical, and are more prominent on the face and extremities. The pustules are round, firm, and deeply embedded in the skin. After 8 to 9 days, the pustules form a crust, and later, the scab separates from the skin, leaving a pitted scar. In fatal cases, death results from encephalitis, extensive bleeding, or secondary infection.
- Spinal neoplasm (benign). Spinal neoplasm typically causes severe, localized back pain and scoliosis.
- Spinal stenosis. Resembling a ruptured intervertebral disk, spinal stenosis produces back pain with or without sciatica, which commonly affects both legs. The pain may radiate to the toes and may progress to numbness or weakness unless the patient rests.
- Spondylolisthesis. A major structural disorder characterized by forward slippage of one vertebra onto another, spondylolisthesis may be asymptomatic or may cause low back pain, with or without nerve root involvement. Associated symptoms of nerve root involvement include paresthesia, buttock pain, and pain radiating down the leg. Palpation of the lumbar spine may reveal a “step-off” of the spinous process. Flexion of the spine may be limited.
- Transverse process fracture. Transverse process fracture causes severe localized back pain with muscle spasm and hematoma.
- Vertebral compression fracture. Initially, vertebral compression fracture may be painless. Several weeks later, it causes back pain aggravated by weight bearing and local tenderness. Fracture of a thoracic vertebra may cause referred pain in the lumbar area.
- Vertebral osteomyelitis. Initially, vertebral osteomyelitis causes insidious back pain. As it progresses, the pain may become constant, more pronounced at night, and aggravated by spinal movement. Accompanying signs and symptoms include vertebral and hamstring spasms, tenderness of the spinous processes, fever, and malaise.
- Vertebral osteoporosis. Vertebral osteoporosis causes chronic, aching back pain that is aggravated by activity and somewhat relieved by rest. Tenderness may also occur.
Other Causes
- Neurologic tests. Lumbar puncture and myelography can produce transient back pain.
Special Considerations
Monitor the patient closely if the back pain suggests a life-threatening cause. Be alert for increasing pain, altered neurovascular status in the legs, loss of bowel or bladder control, altered vital signs, sweating, and cyanosis.
Until a tentative diagnosis is made, withhold analgesics, which may mask the symptoms of a life-threatening cause. Also, withhold food and fluids in case surgery is necessary. Make the patient as comfortable as possible by elevating the head of the bed and placing a pillow under his knees. Encourage relaxation techniques such as deep breathing. Prepare the patient for a rectal or pelvic examination. He may also require routine blood tests, urinalysis, a computed tomography scan, appropriate biopsies, and X-rays of the chest, abdomen, and spine.
Fit the patient for a corset or lumbosacral support. Instruct him not to wear this in bed. He may also require heat or cold therapy, a backboard, a convoluted foam mattress, or pelvic traction. Explain these pain-relief measures to the patient. Teach him about alternatives to analgesic drug therapy, such as biofeedback and transcutaneous electrical nerve stimulation.
Be aware that back pain is notoriously associated with malingering. Refer the patient to other professionals, such as a physical therapist, an occupational therapist, or a psychologist, if indicated.
Patient Counseling
Provide information about the use of anti-inflammatories, analgesics, and alternatives to drug therapy, such as biofeedback and transcutaneous electric nerve stimulation. Teach relaxation techniques such as deep breathing, and instruct the patient on correct use of corset or lumbosacral support. Discuss lifestyle changes, such as losing weight or correcting posture.
Pediatric Pointers
Because a child may have difficulty describing back pain, be alert for nonverbal clues, such as wincing or a refusal to walk. Closely observe family dynamics during history taking for clues that suggest child abuse.
Back pain in the child may stem from intervertebral disk inflammation (diskitis), neoplasms, idiopathic juvenile osteoporosis, and spondylolisthesis. Disk herniation typically doesn’t cause back pain. Scoliosis, a common disorder in adolescents, rarely causes back pain.
Geriatric Pointers
Suspect metastatic cancer — especially of the prostate, colon, or breast — in older patients with a recent onset of back pain that usually isn’t relieved by rest and worsens at night.
REFERENCES
Costa, L. C., Maher, C. G., McAuley, J. H., Hancock, M. J., Herbert, R. D., Refshauge K. M., & Henschke, N. (2009). Prognosis for patients with chronic low back pain: Inception cohort study. British Medical Journal, 339, b3829.
Hay, E. M., & Dunn, K. M. (2009). Prognosis of low back pain in primary care. British Medical Journal, 339, 816–817.
Battle’s Sign
Battle’s sign — ecchymosis over the mastoid process of the temporal bone — is commonly the only outward sign of a basilar skull fracture. In fact, this type of fracture may go undetected even by skull X-rays. If left untreated, it can be fatal because of associated injury to the nearby cranial nerves and brain stem as well as to blood vessels and the meninges.
Appearing behind one or both ears, Battle’s sign is easily overlooked or hidden by the patient’s hair. During emergency care of a trauma victim, it may be overshadowed by imminently life-threatening or more apparent injuries.
A force that’s strong enough to fracture the base of the skull causes Battle’s sign by damaging supporting tissues of the mastoid area and causing seepage of blood from the fracture site to the mastoid. Battle’s sign usually develops 24 to 36 hours after the fracture and may persist for several days to weeks.
History and Physical Examination
Perform a complete neurologic examination. Begin with the history. Ask the patient about recent trauma to the head. Did he sustain a severe blow to the head? Was he involved in a motor vehicle accident? Note the patient’s level of consciousness as he responds. Does he respond quickly or slowly? Are his answers appropriate, or does he appear confused?
Check the patient’s vital signs; be alert for widening pulse pressure and bradycardia and signs of increased intracranial pressure. Assess cranial nerve function in nerves II, III, IV, VI, VII, and VIII. Evaluate pupillary size and response to light as well as motor and verbal responses. Relate these data to the Glasgow Coma Scale. Also, note cerebrospinal fluid (CSF) leakage from the nose or ears. Ask about postnasal drip, which may reflect CSF drainage down the throat. Look for the halo sign — a bloodstain encircled by a yellowish ring — on bed linens or dressings. To confirm that drainage is CSF, test it with a Dextrostix; CSF is positive for glucose, whereas mucus isn’t. Follow up the neurologic examination with a complete physical examination to detect other injuries associated with basilar skull fracture.
Medical Causes
- Basilar skull fracture. Battle’s sign may be the only outward sign of basilar skull fracture, or it may be accompanied by periorbital ecchymosis (raccoon eyes), conjunctival hemorrhage, nystagmus, ocular deviation, epistaxis, anosmia, a bulging tympanic membrane (from CSF or blood accumulation), visible fracture lines on the external auditory canal, tinnitus, difficulty hearing, facial paralysis, or vertigo.
Special Considerations
Expect a patient with a basilar skull fracture to be on bed rest for several days to weeks. Keep him flat to decrease pressure on dural tears and to minimize CSF leakage. Monitor his neurologic status closely. Avoid nasogastric intubation and nasopharyngeal suction, which may cause cerebral infection. Also, caution the patient against blowing his nose, which may worsen a dural tear.
The patient may need skull X-rays and a computed tomography scan to help confirm basilar skull fracture and to evaluate the severity of head injury. Typically, a basilar skull fracture and associated dural tears heal spontaneously within several days to weeks. However, if the patient has a large dural tear, a craniotomy may be necessary to repair the tear with a graft patch.
Patient Counseling
Explain what diagnostic tests the patient may need along with what activities he should avoid, and emphasize the importance of bed rest. Explain to the patient (or caregivers) what signs and symptoms to look for and report, such as changes in mental status, loss of consciousness (LOC), or breathing. Tell the patient to take acetaminophen for headaches, discuss the prospect of surgery with the patient, and answer his questions and concerns.
Pediatric Pointers
Children who are victims of abuse frequently sustain basilar skull fractures from severe blows to the head. As in adults, Battle’s sign may be the only outward sign of fracture and, perhaps, the only clue to child abuse. If you suspect child abuse, follow facility protocol for reporting the incident.
REFERENCES
Fugate, J. E., Wijdicks, E. F., Mandrekar, J., Claassen, D. O., Manno, E. M., White, R. D., …, Rabinstein, A. A. (2010). Predictors of neurologic outcome in hypothermia after cardiac arrest. Annals of Neurology, 68(6), 907–914.
Perry, J. J., Stiell, I. G., Sivilotti, M. L., Bullard, M. J., Emond, M., Symington, C., …, Wells, G. A. (2011). Sensitivity of computed tomography performed within six hours of onset of headache for diagnosis of subarachnoid haemorrhage: Prospective cohort study. British Medical Journal, 343, d4277.
Biot’s Respirations[Ataxic respirations]
A late and ominous sign of neurologic deterioration, Biot’s respirations are characterized by an irregular and unpredictable rate, rhythm, and depth. This rare breathing pattern may appear abruptly and may reflect increased pressure on the medulla coinciding with brain stem compression.
 EMERGENCY INTERVENTIONS
EMERGENCY INTERVENTIONS
Observe the patient’s breathing pattern for several minutes to avoid confusing Biot’s respirations with other respiratory patterns. (See Identifying Biot’s Respirations.) Assess the patient’s respiratory status and prepare to intubate him and provide mechanical ventilation. Next, take his vital signs, noting especially increased systolic pressure.
Medical Causes
- Brain stem compression. Biot’s respirations are characteristic in brain stem compression, a neurologic emergency. Rapidly enlarging lesions may cause ataxic respirations and lead to complete respiratory arrest.
Special Considerations
Monitor the patient’s vital signs frequently, including oxygen saturation. Elevate the head of the patient’s bed 30 degrees to help reduce intracranial pressure. Prepare the patient for emergency surgery to relieve pressure on the brain stem. Computed tomography scans or magnetic resonance imaging may confirm the cause of brain stem compression.
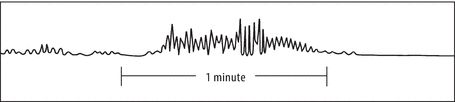
Identifying Biot’s Respirations
Biot’s respirations, also known as ataxic respirations, have a completely irregular pattern. Shallow and deep breaths occur randomly, with haphazard, irregular pauses. The respiratory rate tends to be slow and may progressively decelerate to apnea.
Patient Counseling
Because Biot’s respirations typically reflect a grave prognosis, give the patient’s family information and emotional support.
Pediatric Pointers
Biot’s respirations are rarely seen in children.
REFERENCES
Schefold, J. C., Storm, C., Krüger, A., Ploner, C. J., & Hasper, D. (2009). The Glasgow Coma Score is a predictor of good outcome in cardiac arrest patients treated with therapeutic hypothermia. Resuscitation, 80(6), 658–661.
Wijdicks, E. F. (2010). The bare essentials: Coma. Practical Neurology, 10(1), 51–60.
Bladder Distention
Bladder distention — abnormal enlargement of the bladder — results from an inability to excrete urine, which results in its accumulation. Distention can be caused by a mechanical or anatomic obstruction, neuromuscular disorder, or the use of certain drugs. Relatively common in all ages and both sexes, it’s most common in older men with prostate disorders that cause urine retention.
Distention usually develops gradually, but it occasionally has a sudden onset. Gradual distention usually remains asymptomatic until stretching of the bladder produces discomfort. Acute distention produces suprapubic fullness, pressure, and pain. If severe distention isn’t corrected promptly by catheterization or massage, the bladder rises within the abdomen, its walls become thin, and renal function can be impaired.
Bladder distention is aggravated by the intake of caffeine, alcohol, large quantities of fluid, and diuretics. (See Bladder Distention: Common Causes and Associated Findings, pages 92 and 93.)
 EMERGENCY INTERVENTIONS
EMERGENCY INTERVENTIONS
If the patient has severe distention, insert an indwelling urinary catheter to help relieve discomfort and prevent bladder rupture. If more than 700 mL is emptied from the bladder, compressed blood vessels dilate and may make the patient feel faint. Typically, the indwelling urinary catheter is clamped for 30 to 60 minutes to permit vessel compensation.
History and Physical Examination
If distention isn’t severe, begin by reviewing the patient’s voiding patterns. Find out the time and amount of the patient’s last voiding and the amount of fluid consumed since then. Ask if he has difficulty urinating. Does he use Valsalva’s or Credé’s maneuver to initiate urination? Does he urinate with urgency or without warning? Is urination painful or irritating? Ask about the force and continuity of his urine stream and whether he feels that his bladder is empty after voiding.
Explore the patient’s history of urinary tract obstruction or infections; venereal disease; neurologic, intestinal, or pelvic surgery; lower abdominal or urinary tract trauma; and systemic or neurologic disorders. Note his drug history, including his use of over-the-counter drugs.
Take the patient’s vital signs, and percuss and palpate the bladder. (Remember that if the bladder is empty, it can’t be palpated through the abdominal wall.) Inspect the urethral meatus, and measure its diameter. Describe the appearance and amount of any discharge. Finally, test for perineal sensation and anal sphincter tone; in male patients, digitally examine the prostate gland.
Medical Causes
- Benign prostatic hyperplasia (BPH). With BPH, bladder distention gradually develops as the prostate enlarges. Occasionally, its onset is acute. Initially, the patient experiences urinary hesitancy, straining, and frequency; reduced force of and the inability to stop the urine stream; nocturia; and postvoiding dribbling. As the disorder progresses, it produces prostate enlargement, sensations of suprapubic fullness and incomplete bladder emptying, perineal pain, constipation, and hematuria.
- Bladder calculi. Bladder calculi may produce bladder distention but more commonly produce pain as the only symptom. The pain is usually referred to the tip of the penis, the vulvar area, the lower back, or the heel. It worsens during walking or exercise and abates when the patient lies down. It can be accompanied by urinary frequency and urgency, terminal hematuria, and dysuria. Pain is usually most severe when micturition ceases.
- Bladder cancer. By blocking the urethral orifice, neoplasms can cause bladder distention. Associated signs and symptoms include hematuria (most common sign); urinary frequency and urgency; nocturia; dysuria; pyuria; pain in the bladder, rectum, pelvis, flank, back, or legs; vomiting; diarrhea; and sleeplessness. A mass may be palpable on bimanual examination.
 CULTURAL CUE
CULTURAL CUE
Bladder cancer is twice as common in Whites as in Blacks. It’s relatively uncommon among Asians, Hispanics, and Native Americans.
- Multiple sclerosis. With multiple sclerosis, a neuromuscular disorder, urine retention, and bladder distention result from the interruption of upper motor neuron control of the bladder. Associated signs and symptoms include optic neuritis, paresthesia, impaired position and vibratory senses, diplopia, nystagmus, dizziness, abnormal reflexes, dysarthria, muscle weakness, emotional lability, Lhermitte’s sign (transient, electric-like shocks that spread down the body when the head is flexed), Babinski’s sign, and ataxia.
- Prostate cancer. Prostate cancer eventually causes bladder distention in about 25% of patients. Usual signs and symptoms include dysuria, urinary frequency and urgency, nocturia, weight loss, fatigue, perineal pain, constipation, and induration of the prostate or a rigid, irregular prostate on digital rectal examination. For some patients, urine retention and bladder distention are the only signs.
 CULTURAL CUE
CULTURAL CUE
Prostate cancer is more common in blacks than in other racial or ethnic groups.
- Prostatitis. With acute prostatitis, bladder distention occurs rapidly along with perineal discomfort and suprapubic fullness. Other signs and symptoms include perineal pain; a tense, boggy, tender, and warm enlarged prostate; decreased libido; impotence; decreased force of the urine stream; dysuria; hematuria; and urinary frequency and urgency. Additional signs and symptoms include fatigue, malaise, myalgia, fever, chills, nausea, and vomiting.
With chronic prostatitis, bladder distention is rare. However, it may be accompanied by sensations of perineal discomfort and suprapubic fullness, prostatic tenderness, decreased libido, urinary frequency and urgency, dysuria, pyuria, hematuria, persistent urethral discharge, ejaculatory pain, and a dull pain radiating to the lower back, buttocks, penis, or perineum.
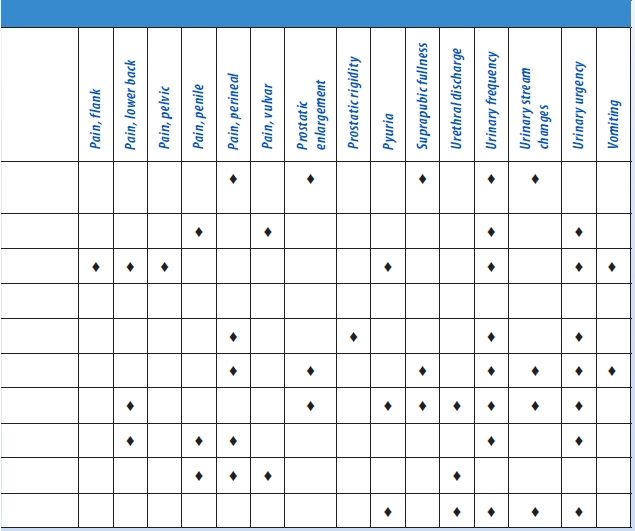
Bladder Distention: Common Causes and Associated Findings
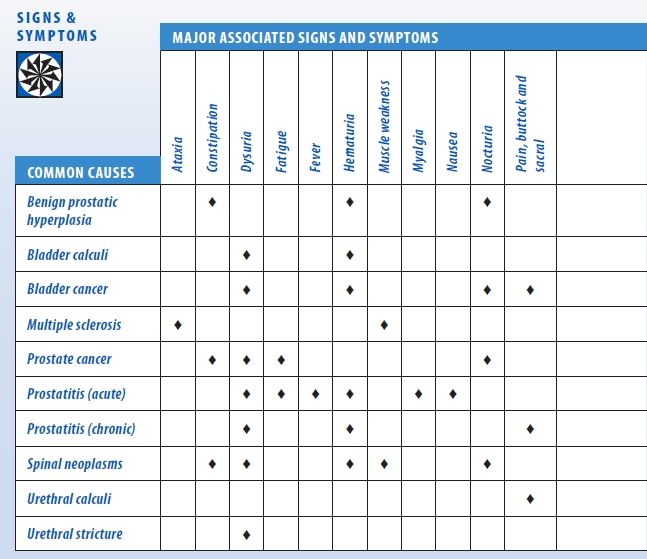
- Spinal neoplasms. Disrupting upper neuron control of the bladder, spinal neoplasms cause neurogenic bladder and resultant distention. Associated signs and symptoms include a sense of pelvic fullness, continuous overflow dribbling, back pain that typically mimics sciatica pain, constipation, tender vertebral processes, sensory deficits, and muscle weakness, flaccidity, and atrophy. Signs and symptoms of urinary tract infection (dysuria, urinary frequency and urgency, nocturia, tenesmus, hematuria, and weakness) may also occur.
- Urethral calculi. With urethral calculi, urethral obstruction leads to bladder distention. The patient experiences interrupted urine flow. The obstruction causes pain radiating to the penis or vulva and referred to the perineum or rectum. It may also produce a palpable stone and urethral discharge.
- Urethral stricture. Urethral stricture results in urine retention and bladder distention with chronic urethral discharge (most common sign), urinary frequency (also common), dysuria, urgency, decreased force and diameter of the urine stream, and pyuria. Urinoma and urosepsis may also develop.
Other Causes
- Catheterization. Using an indwelling urinary catheter can result in urine retention and bladder distention. While the catheter is in place, inadequate drainage due to kinked tubing or an occluded lumen may lead to urine retention. In addition, a misplaced urinary catheter or irritation with catheter removal may cause edema or spasms of the detrusor muscle and the external urethral sphincter, thereby blocking urine outflow.
- Drugs. Parasympatholytics, anticholinergics, ganglionic blockers, sedatives, anesthetics, and opiates can produce urine retention and bladder distention.
Special Considerations
Monitor the patient’s vital signs and the extent of bladder distention. Encourage the patient to change positions to alleviate discomfort. He may require an analgesic.
Prepare the patient for diagnostic tests (such as endoscopy and radiologic studies) to determine the cause of bladder distention. You may need to prepare him for surgery if interventions fail to relieve bladder distention and obstruction prevents catheterization.
Patient Counseling
Teach the patient to use Valsalva’s maneuver or Credé’s method to empty the bladder. Explain how to stimulate voiding.
Pediatric Pointers
Look for urine retention and bladder distention in infants who fail to void normal amounts. (In the first 48 hours of life, infants excrete about 60 mL of urine; during the next week, they excrete about 300 mL of urine daily.) In males, posterior urethral valves, meatal stenosis, phimosis, spinal cord anomalies, bladder diverticula, and other congenital defects may cause urinary obstruction and resultant bladder distention.
REFERENCES
James, N., Hussain, S., Hall, E., et al. (2010). Results of a 2 × 2 phase III randomized trial of synchronous chemoradiotherapy (CRT) compared to radiotherapy (RT) alone and standard vs. reduced high volume RT in muscle invasive bladder cancer (MIBC) (BC2001 CRUK/01/004). International Journal of Radiation Oncology, Biology, Physics, 78(3), S2–S3.
James, N. D., Hussain, S. A., Hall, E., et al. (2012). Radiotherapy with or without chemotherapy in muscle-invasive bladder cancer. New England Journal of Medicine, 366(16), 1477–1488.
Blood Pressure Decrease[Hypotension]
Low blood pressure refers to inadequate intravascular pressure to maintain the oxygen requirements of the body’s tissues. Although commonly linked to shock, this sign may also result from a cardiovascular, respiratory, neurologic, or metabolic disorder. Hypoperfusion states especially affect the kidneys, brain, and heart and may lead to renal failure, a change in the patient’s level of consciousness (LOC), or myocardial ischemia. Low blood pressure may be drug induced or may accompany diagnostic tests — most commonly those using contrast media. It may stem from stress or change of position — specifically, rising abruptly from a supine or sitting position to a standing position (orthostatic hypotension).
Normal blood pressure varies considerably; what qualifies as low blood pressure for one person may be normal for another. Consequently, every blood pressure reading must be compared against the patient’s baseline. Typically, a reading below 90/60 mm Hg, or a drop of 30 mm Hg from the baseline, is considered low blood pressure.
Low blood pressure can reflect an expanded intravascular space (as in severe infections, allergic reactions, or adrenal insufficiency), reduced intravascular volume (as in dehydration and hemorrhage), or decreased cardiac output (as in impaired cardiac muscle contractility). Because the body’s pressure-regulating mechanisms are complex and interrelated, a combination of these factors usually contributes to low blood pressure.
 EMERGENCY INTERVENTIONS
EMERGENCY INTERVENTIONS
If the patient’s systolic pressure is less than 80 mm Hg, or 30 mm Hg below his baseline, suspect shock. Quickly evaluate the patient for a decreased LOC. Check his apical pulse for tachycardia and his respirations for tachypnea. Also, inspect the patient for cool, clammy skin. Elevate the patient’s legs above the level of his heart, or place him in Trendelenburg’s position if the bed can be adjusted. Then, start an I.V. line using a large-bore needle to replace fluids and blood or to administer drugs. Prepare to administer oxygen with mechanical ventilation, if necessary. Monitor the patient’s intake and output, and insert an indwelling urinary catheter to accurately measure urine output. The patient may also need a central venous line or a pulmonary artery catheter to facilitate monitoring his fluid status. Prepare for cardiac monitoring to evaluate cardiac rhythm. Be ready to insert a nasogastric tube to prevent aspiration in the comatose patient. Throughout emergency interventions, keep the patient’s spinal column immobile until spinal cord trauma is ruled out.
History and Physical Examination
If the patient is conscious, ask him about associated symptoms. For example, does he feel unusually weak or fatigued? Has he had nausea, vomiting, or dark or bloody stools? Is his vision blurred? Is his gait unsteady? Does he have palpitations? Does he have chest or abdominal pain or difficulty breathing? Has he had episodes of dizziness or fainting? Do these episodes occur when he stands up suddenly? If so, take the patient’s blood pressure while he’s lying down, sitting, and then standing; compare readings. (See Ensuring Accurate Blood Pressure Measurement, page 96.) A drop in systolic or diastolic pressure of 10 to 20 mm Hg or more and an increase in heart rate of more than 15 beats/minute between position changes suggest orthostatic hypotension.
Next, continue with a physical examination. Inspect the skin for pallor, sweating, and clamminess. Palpate peripheral pulses. Note paradoxical pulse — an accentuated fall in systolic pressure during inspiration — which suggests pericardial tamponade. Then, auscultate for abnormal heart sounds (gallops, murmurs), rate (bradycardia, tachycardia), or rhythm. Auscultate the lungs for abnormal breath sounds (diminished sounds, crackles, wheezing), rate (bradypnea, tachypnea), or rhythm (agonal or Cheyne-Stokes respirations). Look for signs of hemorrhage, including visible bleeding and palpable masses, bruising, and tenderness. Assess the patient for abdominal rigidity and rebound tenderness; auscultate for abnormal bowel sounds. Also, carefully assess the patient for possible sources of infection such as open wounds.
Medical Causes
- Acute adrenal insufficiency. Orthostatic hypotension is characteristic with acute adrenal insufficiency, accompanied by fatigue, weakness, nausea, vomiting, abdominal discomfort, weight loss, fever, and tachycardia. The patient may also have hyperpigmentation of fingers, nails, nipples, scars, and body folds; pale, cool, clammy skin; restlessness; decreased urine output; tachypnea; and coma.
- Alcohol toxicity. Low blood pressure occurs infrequently; more commonly, alcohol toxicity produces distinct alcohol breath odor, tachycardia, bradypnea, hypothermia, a decreased LOC, seizures, a staggering gait, nausea, vomiting, diuresis, and slow, stertorous breathing.
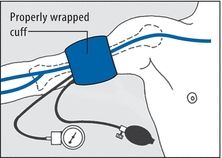
 EXAMINATION TIP Ensuring Accurate Blood Pressure Measurement
EXAMINATION TIP Ensuring Accurate Blood Pressure Measurement
When taking the patient’s blood pressure, begin by applying the cuff properly, as shown here.
Then, be alert for these common pitfalls to avoid recording an inaccurate blood pressure measurement.
- Wrong-sized cuff. Select the appropriate-sized cuff for the patient. This ensures that adequate pressure is applied to compress the brachial artery during cuff inflation. If the cuff bladder is too narrow, a false-high reading will be obtained; too wide, a false-low reading. The cuff bladder width should be about 40% of the circumference of the midpoint of the limb; bladder length should be twice the width. If the arm circumference is less than 13” (33 cm), select a regular-sized cuff; if it’s between 13” and 16” (33 to 40.5 cm), a large-sized cuff; if it’s more than 16”, a thigh cuff. Pediatric cuffs are also available.
- Slow cuff deflation, causing venous congestion in the extremity. Don’t deflate the cuff more slowly than 2 mm Hg/heartbeat because you’ll get a false-high reading.
- Cuff wrapped too loosely, reducing its effective width. Tighten the cuff to avoid a false-high reading.
- Mercury column not read at eye level. Read the mercury column at eye level. If the column is below eye level, you may record a false-low reading; if it’s above eye level, a false-high reading.
- Tilted mercury column. Keep the mercury column vertical to avoid a false-high reading.
- Poorly timed measurement. Don’t take the patient’s blood pressure if he appears anxious or has just eaten or ambulated; you’ll get a false-high reading.
- Incorrect position of the arm. Keep the patient’s arm level with his heart to avoid a false-low reading.
- Cuff overinflation, causing venospasm or pain. Don’t overinflate the cuff because you’ll get a false-high reading.
- Failure to notice an auscultatory gap (sound fades out for 10 to 15 mm Hg, then returns). To avoid missing the top Korotkoff sound, estimate systolic pressure by palpation first. Then, inflate the cuff rapidly — at a rate of 2 to 3 mm Hg/second — to about 30 mm Hg above the palpable systolic pressure.
- Inaudibility of feeble sounds. Before reinflating the cuff, have the patient raise his arm to reduce venous pressure and amplify low-volume sounds. After inflating the cuff, lower the patient’s arm; then, deflate the cuff and listen. Alternatively, with the patient’s arm positioned at heart level, inflate the cuff and have the patient make a fist. Have him rapidly open and close his hand 10 times before you begin to deflate the cuff, and then listen. Make sure to document that the blood pressure reading was augmented.
- Anaphylactic shock. Following exposure to an allergen, such as penicillin or insect venom, a dramatic fall in blood pressure and narrowed pulse pressure signal anaphylactic reaction. Initially, anaphylactic shock causes anxiety, restlessness, a feeling of doom, intense itching (especially of the hands and feet), and pounding headache. Later, it may also produce weakness, sweating, nasal congestion, coughing, difficulty breathing, nausea, abdominal cramps, involuntary defecation, seizures, flushing, change or loss of voice due to laryngeal edema, urinary incontinence, and tachycardia.
- Anthrax (inhalation). Anthrax is an acute infectious disease that’s caused by the gram-positive, spore-forming bacterium Bacillus anthracis. Although the disease most commonly occurs in wild and domestic grazing animals, such as cattle, sheep, and goats, the spores can live in the soil for many years. The disease can occur in humans exposed to infected animals, tissue from infected animals, or biological warfare. Most natural cases occur in agricultural regions worldwide. Anthrax may occur in the cutaneous, inhalation, or GI form.
Inhalation anthrax is caused by inhalation of aerosolized spores. Initial signs and symptoms are flulike and include fever, chills, weakness, cough, and chest pain. The disease generally occurs in two stages with a period of recovery after the initial signs and symptoms. The second stage develops abruptly with rapid deterioration marked by fever, dyspnea, stridor, and hypotension, generally leading to death within 24 hours. Radiologic findings include mediastinitis and symmetric mediastinal widening.
- Cardiac arrhythmias. With an arrhythmia, blood pressure may fluctuate between normal and low readings. Dizziness, chest pain, difficulty breathing, light-headedness, weakness, fatigue, and palpitations may also occur. Auscultation typically reveals an irregular rhythm and a pulse rate greater than 100 beats/minute or less than 60 beats/minute.
- Cardiac contusion. With cardiac contusion, low blood pressure occurs along with tachycardia and, at times, anginal pain and dyspnea.
- Cardiac tamponade. An accentuated fall in systolic pressure (more than 10 mm Hg) during inspiration, known as paradoxical pulse, is characteristic in patients with cardiac tamponade. This disorder also causes restlessness, cyanosis, tachycardia, jugular vein distention, muffled heart sounds, dyspnea, and Kussmaul’s sign (increased venous distention with inspiration).
- Cardiogenic shock. A fall in systolic pressure to less than 80 mm Hg or to 30 mm Hg less than the patient’s baseline because of decreased cardiac contractility is characteristic in patients with cardiogenic shock. Accompanying low blood pressure are tachycardia, narrowed pulse pressure, diminished Korotkoff sounds, peripheral cyanosis, and pale, cool, clammy skin. Cardiogenic shock also causes restlessness and anxiety, which may progress to disorientation and confusion. Associated signs and symptoms include angina, dyspnea, jugular vein distention, oliguria, ventricular gallop, tachypnea, and a weak, rapid pulse.
- Cholera. This acute infection, caused by the bacterium Vibrio cholerae, may be mild with uncomplicated diarrhea or severe and life threatening. Cholera is spread by ingesting contaminated water or food, especially shellfish. Signs include abrupt watery diarrhea and vomiting. Severe fluid and electrolyte loss leads to thirst, weakness, muscle cramps, decreased skin turgor, oliguria, tachycardia, and hypotension. Without treatment, death can occur within hours.
- Diabetic ketoacidosis. Hypovolemia triggered by osmotic diuresis in hyperglycemia is responsible for the low blood pressure associated with diabetic ketoacidosis, which is usually present in patients with type 1 diabetes mellitus. It also commonly produces polydipsia, polyuria, polyphagia, dehydration, weight loss, abdominal pain, nausea, vomiting, breath with fruity odor, Kussmaul’s respirations, tachycardia, seizures, confusion, and stupor that may progress to coma.
- Heart failure. With heart failure, blood pressure may fluctuate between normal and low readings. However, a precipitous drop in blood pressure may signal cardiogenic shock. Other signs and symptoms of heart failure include exertional dyspnea, dyspnea of abrupt or gradual onset, paroxysmal nocturnal dyspnea or difficulty breathing in the supine position (orthopnea), fatigue, weight gain, pallor or cyanosis, sweating, and anxiety. Auscultation reveals ventricular gallop, tachycardia, bilateral crackles, and tachypnea. Dependent edema, jugular vein distention, increased capillary refill time, and hepatomegaly may also occur.
- Hyperosmolar hyperglycemic nonketotic syndrome (HHNS). HHNS, which is common in the patient with type 2 diabetes mellitus, decreases blood pressure — at times dramatically — if he loses significant fluid from diuresis due to severe hyperglycemia and hyperosmolarity. It also produces dry mouth, poor skin turgor, tachycardia, confusion progressing to coma, and, occasionally, generalized tonic-clonic seizure.
- Hypovolemic shock. A fall in systolic pressure to less than 80 mm Hg or 30 mm Hg less than the patient’s baseline, secondary to acute blood loss or dehydration, is characteristic in hypovolemic shock. Accompanying it are diminished Korotkoff sounds, a narrowed pulse pressure, and a rapid, weak, and irregular pulse. Peripheral vasoconstriction causes cyanosis of the extremities and pale, cool, clammy skin. Other signs and symptoms include oliguria, confusion, disorientation, restlessness, and anxiety.
- Hypoxemia. Initially, blood pressure may be normal or slightly elevated, but as hypoxemia becomes more pronounced, blood pressure drops. The patient may also display tachycardia, tachypnea, dyspnea, and confusion and may progress from stupor to coma.
- Myocardial infarction (MI). With MI, a life-threatening disorder, blood pressure may be low or high. However, a precipitous drop in blood pressure may signal cardiogenic shock. Associated signs and symptoms include chest pain that may radiate to the jaw, shoulder, arm, or epigastrium; dyspnea; anxiety; nausea or vomiting; sweating; and cool, pale, or cyanotic skin. Auscultation may reveal an atrial gallop, a murmur and, occasionally, an irregular pulse.
- Neurogenic shock. The result of sympathetic denervation due to cervical injury or anesthesia, neurogenic shock produces low blood pressure and bradycardia. However, the patient’s skin remains warm and dry because of cutaneous vasodilation and sweat gland denervation. Depending on the cause of shock, there may also be motor weakness of the limbs or diaphragm.
- Pulmonary embolism. Pulmonary embolism causes sudden, sharp chest pain and dyspnea accompanied by a cough and, occasionally, a low-grade fever. Low blood pressure occurs with a narrowed pulse pressure and diminished Korotkoff sounds. Associated signs include tachycardia, tachypnea, a paradoxical pulse, jugular vein distention, and hemoptysis.
- Septic shock. Initially, septic shock produces fever and chills. Low blood pressure, tachycardia, and tachypnea may also develop early, but the patient’s skin remains warm. Later, low blood pressure becomes increasingly severe — less than 80 mm Hg or 30 mm Hg less than the patient’s baseline — and is accompanied by narrowed pulse pressure. Other late signs and symptoms include pale skin, cyanotic extremities, apprehension, thirst, oliguria, and coma.
- Vasovagal syncope. Vasovagal syncope is the transient loss or near loss of consciousness following stressful, painful, or claustrophobic experiences. It’s characterized by low blood pressure, pallor, cold sweats, nausea, palpitations or slowed heart rate, and weakness.
Other Causes
- Diagnostic tests. Diagnostic tests include the gastric acid stimulation test using histamine and X-ray studies using contrast media. The latter may trigger an allergic reaction, which causes low blood pressure.
- Drugs. Calcium channel blockers, diuretics, vasodilators, alpha- and beta-adrenergic blockers, general anesthetics, opioid analgesics, monoamine oxidase inhibitors, anxiolytics (such as benzodiazepines), tranquilizers, and most I.V. antiarrhythmics (especially bretylium tosylate) can cause low blood pressure.
Special Considerations
Check the patient’s vital signs frequently to determine if low blood pressure is constant or intermittent. If blood pressure is extremely low, an arterial catheter may be inserted to allow close monitoring of pressures. Alternatively, a Doppler flowmeter may be used.
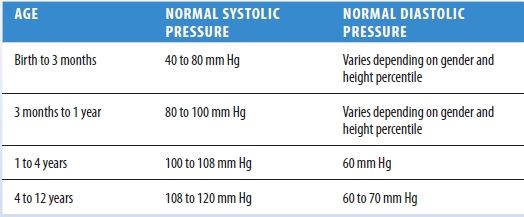
Normal Pediatric Blood Pressure
If the patient is symptomatic, place him on bed rest and keep the side rails of the bed up. If the patient is asymptomatic and ambulatory, assist him as necessary. To avoid falls, don’t leave a hypotensive patient unattended when he’s sitting or walking.
Prepare the patient for laboratory tests, which may include urinalysis, routine blood studies, an electrocardiogram, and chest, cervical, and abdominal X-rays.
Patient Counseling
Advise the patient with orthostatic hypotension to stand up slowly from a sitting or lying position, and emphasize the importance of dangling the feet and rising slowly when getting out of bed. For patients with vasovagal syncope, discuss how to avoid triggers. Also, discuss the need for a cane or a walker.
Pediatric Pointers
Normal blood pressure in children is lower than that in adults. (See Normal Pediatric Blood Pressure.)
Because accidents occur frequently in children, suspect trauma or shock first as a possible cause of low blood pressure. Remember that low blood pressure typically doesn’t accompany head injury in adults because intracranial hemorrhage is insufficient to cause hypovolemia. However, it does accompany head injury in infants and young children; their expandable cranial vaults allow significant blood loss into the cranial space, resulting in hypovolemia.
Another common cause of low blood pressure in children is dehydration, which results from failure to thrive or from persistent diarrhea and vomiting for as little as 24 hours.
Geriatric Pointers
In elderly patients, low blood pressure commonly results from the use of multiple drugs with this potential adverse effect, a problem that needs to be addressed. Orthostatic hypotension due to autonomic dysfunction is another common cause.
REFERENCES
Fan, C. W., Walsh, C., & Cunningham, C. J. (2011). The effect of sleeping with the head of the bed elevated six inches on elderly patients with orthostatic hypotension: An open randomised controlled trial. Age and Ageing, 40, 187–192.
Freeman, R., Wieling, W., Axelrod, F. B., Benditt, D. G., Benarroch, E., Biaggioni, I., … van Dijk, J. G. (2011). Consensus statement on the definition of orthostatic hypotension, neurally medicated syncope and the postural tachycardia syndrome. Clinical Autonomic Research, 21, 69–72.
Blood Pressure Increase[Hypertension]
Elevated blood pressure — an intermittent or sustained increase in blood pressure exceeding 140/90 mm Hg — strikes more men than women and twice as many Blacks as Whites. By itself, this common sign is easily ignored by the patient; after all, he can’t see or feel it. However, its causes can be life threatening.
 GENDER CUE
GENDER CUE
Hypertension has been reported to be two to three times more common in women taking hormonal contraceptives than those not taking them. Women age 35 and older who smoke cigarettes should be strongly encouraged to stop; if they continue to smoke, they should be discouraged from using hormonal contraceptives.
Elevated blood pressure may develop suddenly or gradually. A sudden, severe rise in pressure (exceeding 180/110 mm Hg) may indicate life-threatening hypertensive crisis. However, even a less dramatic rise may be equally significant if it heralds a dissecting aortic aneurysm, increased intracranial pressure, myocardial infarction, eclampsia, or thyrotoxicosis.
Usually associated with essential hypertension, elevated blood pressure may also result from a renal or endocrine disorder; a treatment that affects fluid status, such as dialysis; or a drug’s adverse effect. Ingestion of large amounts of certain foods, such as black licorice and cheddar cheese, may temporarily elevate blood pressure. (See Pathophysiology of Elevated Blood Pressure.)
Sometimes, elevated blood pressure may simply reflect inaccurate blood pressure measurement. (See Ensuring Accurate Blood Pressure Measurement, page 96.) However, careful measurement alone doesn’t ensure a clinically useful reading. To be useful, each blood pressure reading must be compared with the patient’s baseline. Also, serial readings may be necessary to establish elevated blood pressure.
Pathophysiology of Elevated Blood Pressure
Blood pressure — the force blood exerts on vessels as it flows through them — depends on cardiac output, peripheral resistance, and blood volume. A brief review of its regulating mechanisms — nervous system control, capillary fluid shifts, kidney excretion, and hormonal changes — will help you understand how elevated blood pressure develops.
- Nervous system control involves the sympathetic system, chiefly baroreceptors and chemoreceptors, which promotes moderate vasoconstriction to maintain normal blood pressure. When this system responds inappropriately, increased vasoconstriction enhances peripheral resistance, resulting in elevated blood pressure.
- Capillary fluid shifts regulate blood volume by responding to arterial pressure. Increased pressure forces fluid into the interstitial space; decreased pressure allows it to be drawn back into the arteries by osmosis. However, this fluid shift may take several hours to adjust blood pressure.
- Kidney excretion also helps regulate blood volume by increasing or decreasing urine formation. Normally, an arterial pressure of about 60 mm Hg maintains urine output. When pressure drops below this reading, urine formation ceases, thereby increasing blood volume. Conversely, when arterial pressure exceeds this reading, urine formation increases, thereby reducing blood volume. Like capillary fluid shifts, this mechanism may take several hours to adjust blood pressure.
- Hormonal changes reflect stimulation of the kidney’s renin-angiotensin-aldosterone system in response to low arterial pressure. This system affects vasoconstriction, which increases arterial pressure, and stimulates aldosterone release, which regulates sodium retention — a key determinant of blood volume.
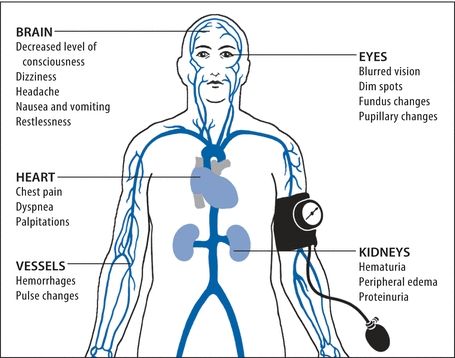
Elevated blood pressure signals the breakdown or inappropriate response of these pressure-regulating mechanisms. Its associated signs and symptoms concentrate in the target organs and tissues illustrated below.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


