Dermoscopy: Introduction
Dermoscopy allows the clinician to visualize structures below the level of the stratum corneum. These structures are not routinely discernible without dermoscopy. The presence or absence of specific dermoscopic structures, their location and their distribution can assist the clinician in making a diagnosis or at least in narrowing the differential diagnosis.
The major goal of dermoscopy is to differentiate benign from malignant lesions on the skin so that one is less likely to miss a skin cancer (higher sensitivity) and less likely to perform unnecessary biopsies (higher specificity). Together, this will increase your diagnostic accuracy.
Polarized
Nonpolarized
Hybrid, which combines a polarized mode with a nonpolarized mode in one dermatoscope.
Because some structures are better seen under polarized light and others best seen without polarization is helpful to purchase a hybrid dermatoscope. Dermatoscopes are currently manufactured by 3Gen, Welch Allyn, Canfield and Heine (Figures C-1 and C-2). A number of dermatoscopes work well while attached to the iPhone for easy image capture and full screen images that can be shown to the patients.


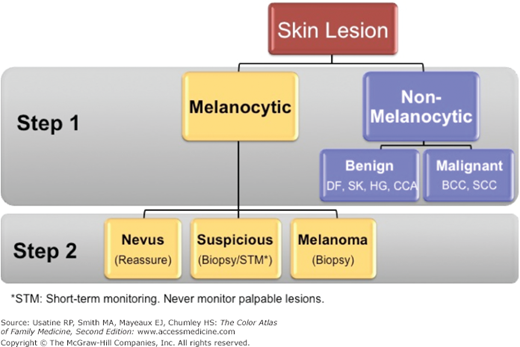
Step 1 requires the observer to decide whether the lesion in question is of melanocytic origin (contains melanocytes and therefore could be a melanoma). If the lesion is deemed to be a melanocytic lesion then the observer proceeds to step 2. In this phase of the evaluation, the observer needs to decide whether the lesion is a benign nevus or a melanoma. However, if during step 1 analysis the lesion does not display any features of a melanocytic lesion then the observer needs to decide if the lesion possesses any criteria for a basal cell carcinoma, seborrheic keratosis, hemangioma, or dermatofibroma. If the lesion does not display any structures common to the aforementioned lesions then the lesion is considered nondescript or featureless. The index of suspicion needs to remain high for all featureless lesions as amelanotic melanoma can present as a completely structureless lesion. These featureless lesions sometimes do reveal blood vessels and, if present, their morphology can often help in narrowing the differential diagnosis.
Step 1 – Level 1
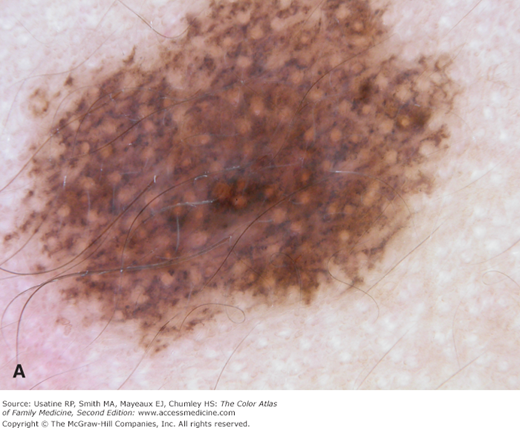
- a. Pigment network (Figure C-4).
- b. Negative network (Figure C-5).
- c. Streaks (Figure C-6).
- d. Homogeneous blue pigmentation (Figure C-7).
- e. Aggregated globules (Figure C-8).
- f. Pseudonetwork (facial skin) (Figure C-9).
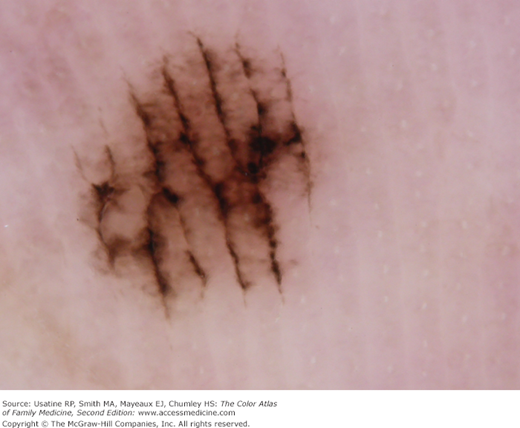
- g. Parallel pigment pattern (acral lesions) (Figure C-10).
- h. There is one exception to including lesions with pigment network in the melanocytic category; that is, the dermatofibroma in which the pattern trumps the network (Figure C-11).

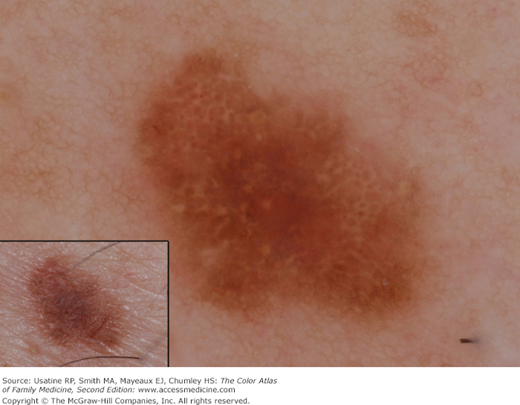
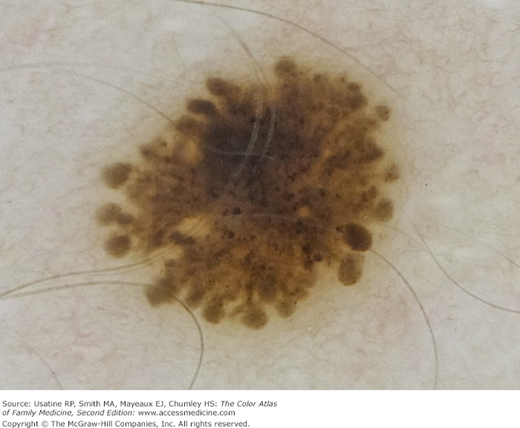
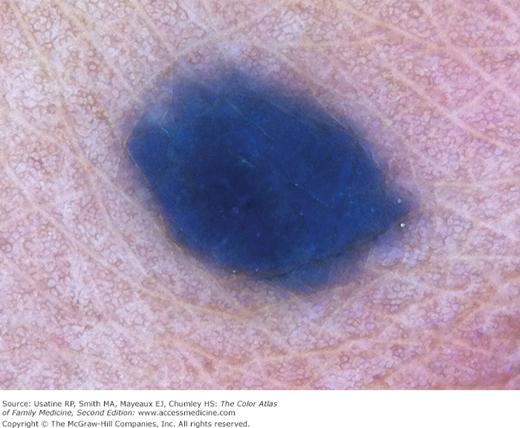
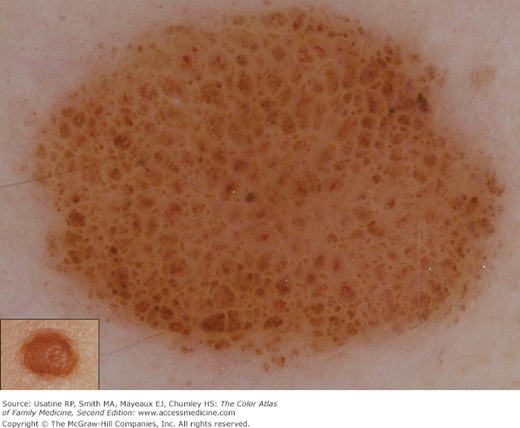
Figure C-9
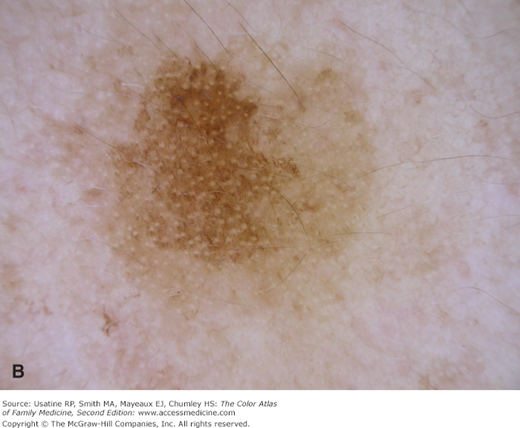
Pseudonetwork is the net-like pattern made by white adnexal openings on the face within any pigmented lesion. A. Pseudonetwork pattern is seen on the face in this congenital nevus that is melanocytic. B. Although this solar lentigo also has a pseudonetwork pattern created by white adnexal openings it is not melanocytic. It does have a typical moth-eaten border found in solar lentigines and seborrheic keratoses. (Courtesy of Richard P. Usatine, MD.)

This lesion does not display any of the structures commonly seen in melanocytic lesions (i.e., network, streaks, globules). It also does not have any features of a basal cell carcinoma, seborrheic keratosis, dermatofibroma, or hemangioma. Thus, this is a featureless lesion. However, it does display many irregular tortuous blood vessels, which may be a sign of neoangiogenesis. The possibility of melanoma needs to be entertained for such featureless lesion.
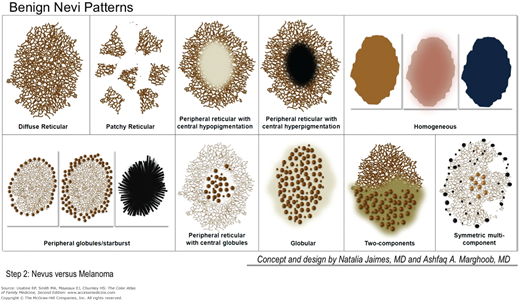
Step 2
- If the lesion is deemed to be of melanocytic origin, then one needs to decide whether the lesion is a benign nevus or a melanoma.
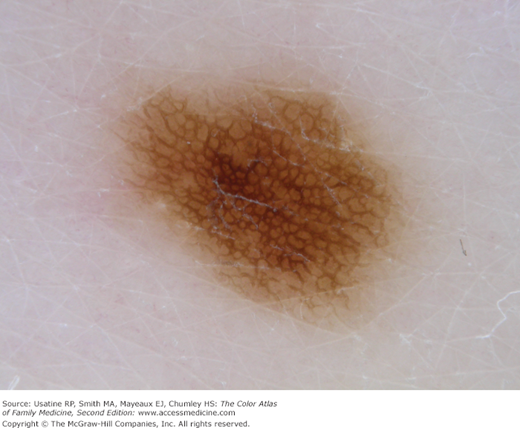
Diffuse reticular (Figure C-13)
Patchy reticular (Figure C-14)
Peripheral reticular with central hypopigmentation (Figure C-15)
Peripheral reticular with central hyperpigmentation (Figure C-16)
Homogeneous (Figure C-17)
Peripheral globules/starburst (Figure C-18)
Peripheral reticular with central globules (Figure C-19)
Globular (Figure C-20)
Two-component (Figure C-21)
Symmetric multicomponent (note this pattern should be interpreted with caution and a biopsy is probably warranted for dermoscopic novices) (Figure C-22)