Interpreting Evidence-Based Medicine
Strength of Recommendation (SOR) | Definition |
|---|---|
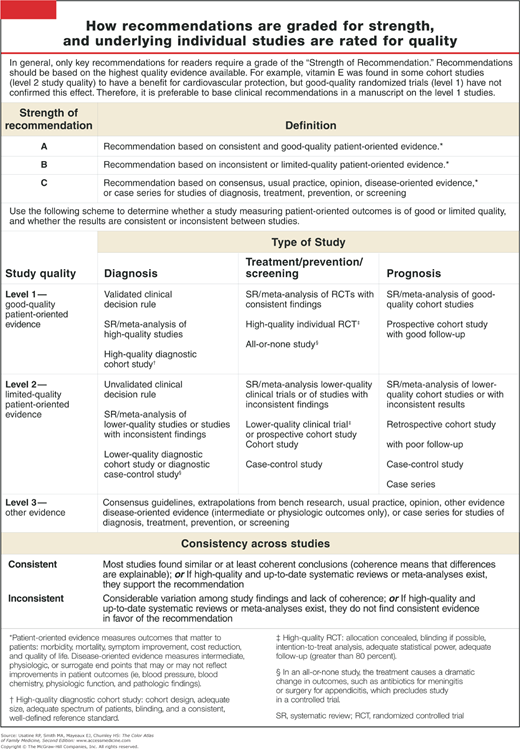
A | Recommendation based on consistent and good-quality patient-oriented evidence. |
B | Recommendation based on inconsistent or limited-quality patient-oriented evidence. |
C | Recommendation based on consensus, usual practice, opinion, disease-oriented evidence, or case series for studies of diagnosis, treatment, prevention, or screening. |
“Evidence-based medicine—is this something new?” asked my father, incredulously. “What were you practicing before?”
Like my father, our patients assume that we provide recommendations to them based on scientific evidence. The idea that there might not be relevant evidence or that we might not have access to that evidence has not even occurred to most of them. This is certainly not to imply that such evidence is the be-all and end-all of medical practice or that our patients would follow such recommendations blindly—rather, for me, it is a starting point from which to begin rational testing or outline a possible therapeutic plan.
The first time that I recall the term evidence-based medicine (EBM) being discussed was in the early 1990s.1,2 It seemed that we would need to develop skills in evaluating the published literature and determining its quality, validity, and relevance to the care of our patients. As a teacher and researcher, I was intrigued by the challenges of critically appraising articles and teaching this newfound skill to others. As a clinician, however, I was most interested in answering clinical questions and doing so in a compressed time frame. I need rapid access to tools or sources that provided summary answers to those questions tagged to information about the quantity and quality of the evidence and the consistency of information across studies.
There seemed to be many systems for rating literature but few that met the needs of the busy practitioner trying to make sense of individual clinical trials and the hundreds of both evidence-based and consensus-based guidelines that seemed to spring up overnight. In 2004, the editors of the U.S. family medicine and primary care journals and the Family Practice Inquiries Network published a paper on a unified taxonomy called Strength of Recommendation (SOR) Taxonomy that seemed to fit the bill (Figure A-1).3 This taxonomy made use of existing systems for judging study quality while incorporating the concept of patient-oriented (e.g., mortality, morbidity, symptom improvement) rather than disease-oriented (e.g., change in blood pressure, blood chemistry) outcomes as most relevant. A SOR A recommendation is one based on consistent, good-quality patient-oriented evidence; SOR B is a recommendation based on inconsistent or limited-quality patient-oriented evidence; and SOR C is a recommendation based on consensus, usual practice, opinion, disease- oriented evidence, or case series (Figure A-1 and A-2).