May be indistinguishable histologically and immunohistochemically from apocrine carcinoma
• Primary cutaneous adenoid cystic carcinoma
Cribriform pattern within islands that are relatively uniform in size/shape and not interconnected
Deeply infiltrative, almost always with perineural invasion
• Tubular apocrine adenoma
Well circumscribed, noninfiltrative
Tubular islands with evidence of decapitation secretion
Islands not crowded together
Minimal cytologic atypia
Often myoepithelial cell layer present
• Hidradenocarcinoma
Larger solid and cystic nodules, infiltrative
Admixture of cell types: Clear, squamoid, poroid, mucinous
Hyalinized stroma
Apocrine Carcinoma at Scanning Magnification Low magnification shows a densely cellular dermal proliferation of packed glands and ductal structures, with many lumina easily identified.
Apocrine Carcinoma With Prominent Snouts and Secretions Higher magnification of the ductal/glandular structures shows enlarged, cuboidal to columnar-shaped cells with prominent apical snouts and secretions , typical of apocrine differentiation.
Apocrine Carcinoma With Perineural Invasion High-magnification view of apocrine carcinoma with perineural invasion shows glands lined by cuboidal cells surrounding a nerve. Focal snouts and secretions of cytoplasm are present within the lumina.
Immunohistochemistry for GCDFP-15 Apocrine carcinoma stains diffusely with GCDFP-15. The islands are crowded together, and lumina can be seen in many of the islands.
TERMINOLOGY
Synonyms
• Cribriform apocrine carcinoma
Definitions
• Malignant tumor with apocrine differentiation
CLINICAL ISSUES
Site
• Axilla and anogenital regions are most common sites, but other sites described
Presentation
• Dermal nodule, often asymptomatic
• May present within nevus sebaceus
• No history of breast carcinoma
Treatment
• Wide local excision; role of chemotherapy or radiotherapy unclear
Only gold members can continue reading. Log In or Register to continue











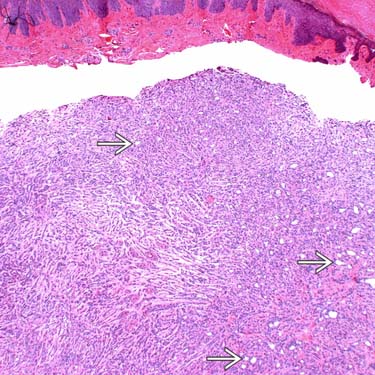
 easily identified.
easily identified.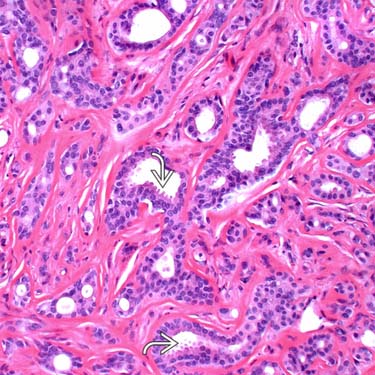
 , typical of apocrine differentiation.
, typical of apocrine differentiation.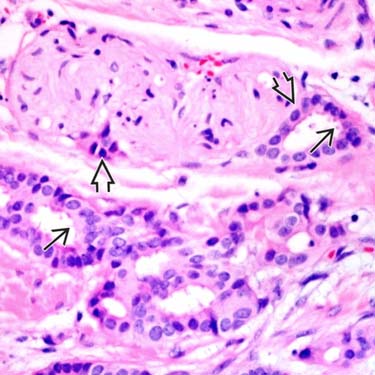
 shows glands lined by cuboidal cells surrounding a nerve. Focal snouts and secretions of cytoplasm
shows glands lined by cuboidal cells surrounding a nerve. Focal snouts and secretions of cytoplasm  are present within the lumina.
are present within the lumina.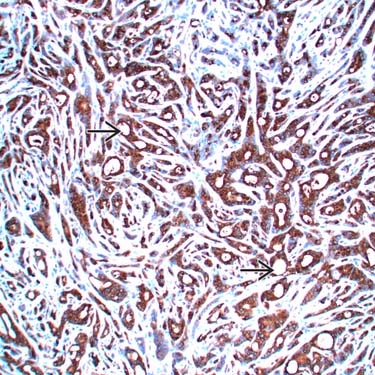
 can be seen in many of the islands.
can be seen in many of the islands.


