Chapter 69 This chapter discusses the use of antiviral drugs and common antiprotozoal medications in primary care. This chapter does not discuss the use of antiviral drugs in the treatment of patients with HIV. The antiherpetic drugs acyclovir, famciclovir, and valacyclovir are closely related. They are used in the treatment of initial and recurrent (i.e., more than six outbreaks per year) mucosal and cutaneous herpes simplex types 1 and 2, and for the treatment of acute herpes simplex virus (HSV) infection. Acyclovir has the greatest antiviral activity in vitro against herpes simplex virus type 1, followed in decreasing order of potency by HSV type 2 (HSV-2), varicella-zoster virus, Epstein-Barr virus, and cytomegalovirus. Penciclovir is structurally similar but is used only topically (see Chapter 13). Amantadine, rimantadine, zanamivir, and oseltamivir are used for the prevention and treatment of influenza virus infection although the effectiveness of oseltamivir has been called into question with new data. Amantadine is also used in Parkinson’s disease (see Chapter 46). Amantadine and rimantadine are similar, as are oseltamivir and zanamivir. Oseltamivir currently is being stockpiled in preparation for an avian influenza pandemic and is not generally available. DNA viruses include herpesviruses (e.g., chickenpox, shingles, herpes), adenoviruses (e.g., conjunctivitis, pharyngitis), hepadna viruses (e.g., hepatitis B), and papillomaviruses (e.g., warts). RNA viruses include rubella (e.g., German measles), rhabdoviruses (e.g., rabies), picornaviruses (e.g., poliomyelitis, meningitis, colds), arboviruses (e.g., yellow fever), orthomyxoviruses (e.g., influenza), and paramyxoviruses (e.g., measles and mumps). The retroviruses are a subgroup of RNA viruses that are discussed in the chapter on antiretroviral medications (see Chapter 68). Several other viruses are discussed in the chapter on immunization and immunity (see Chapter 70). Some of the less common viruses are not described in this text. Acyclovir is a synthetic purine nucleoside analog. Valacyclovir is a prodrug of acyclovir, and famciclovir is a prodrug of penciclovir. (See Chapter 3 for a discussion of prodrugs.) Both have similar mechanisms of action as acyclovir. They work by inhibiting viral DNA synthesis. These drugs are activated by the enzyme thymidine kinase, which is found only in cells that are infected by the virus. Consequently, they are relatively nontoxic to cells that are not infected by the virus. In chemical terms, activation of the antiviral first occurs in the infected cells and is followed by phosphorylation by the enzyme thymidine kinase. Finally, acyclovir triphosphate (i.e., the active derivative obtained from monophosphate by host cell enzymes) inhibits viral DNA polymerase, thereby blocking viral replication. See World Health Organization at www.worldhealthwho/int for specific diseases treatment guidelines. • Oral antivirals are effective in herpes. • Neuraminidase inhibitors are effective in influenza. • Babies with neonatal herpes with CNS involvement show improved neurodevelopmental outcomes at age 1 when given 6 months of oral acyclovir. The treatment also prevents cutaneous recurrences in babies who have neonatal herpes simplex virus involving the skin, eye, or mouth. • Start treatment as soon as possible. • Acyclovir, famciclovir, and valacyclovir all are effective for short-term treatment, long-term suppression, and treatment of recurrences. • Treatment of acute infection does not eliminate chronic infection. • Resistance to amantadine and rimantadine has made them largely ineffective. • Zanamivir is effective against most strains of influenza A and B but generally is not available. Oseltamivir may cut the length of time people have symptoms but may not prevent complications such as pneumonia, although nausea and other adverse effects may have been underreported. Much attention has been focused on the use of metronidazole in the treatment of patients with Helicobacter pylori, an organism involved in the development of gastritis and peptic ulcer disease. Metronidazole, when given in conjunction with bismuth (and sometimes omeprazole or a histamine blocker) an antibiotic and a PPI, appears to be effective in treating H. pylori. The addition of tetracycline may increase the length of remission (see Chapter 27). Monitor closely for toxicity and adverse effects, especially in patients with renal impairment. • metronidazole: Perform total CBC with differential leukocyte counts before and after therapy. • chloroquine: Perform baseline and periodic ophthalmologic examinations every 3 months or with any eye symptoms. • Monitor for muscular weakness, question and examine the patient, and test knee and ankle reflexes.
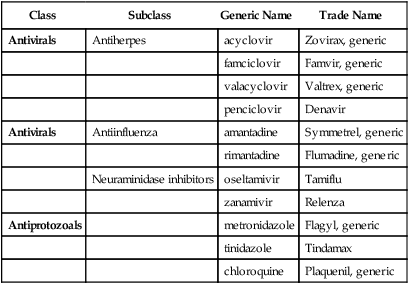
Antivirals and Antiprotozoal Agents
Class
Subclass
Generic Name
Trade Name
Antivirals
Antiherpes
acyclovir
Zovirax, generic
famciclovir
Famvir, generic
valacyclovir
Valtrex, generic
penciclovir
Denavir
Antivirals
Antiinfluenza
amantadine
Symmetrel, generic
rimantadine
Flumadine, generic
Neuraminidase inhibitors
oseltamivir
Tamiflu
zanamivir
Relenza
Antiprotozoals
metronidazole
Flagyl, generic
tinidazole
Tindamax
chloroquine
Plaquenil, generic
Therapeutic Overview of Viruses and Protozoa
Anatomy and Physiology
Virus
Mechanism of Action
Antivirals
Treatment Principles
Standardized Guidelines
Evidence-Based Recommendations
Cardinal Points of Treatment
Antiprotozoal Drugs
Metronidazole
How to Monitor
Antivirals
Antiprotozoals
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Antivirals and Antiprotozoal Agents

Only gold members can continue reading. Log In or Register to continue
