• Peripheral blood with multilobated “flower cells”
• Lymph nodes with effaced architecture & diffuse infiltrate
• Bone marrow with patchy involvement & increased osteoclasts
Ancillary Tests
• Confirmation of HTLV-I infection by serology
• Immunophenotype
Regulatory T cells CD3(+), CD4(+), CD25(+), FOXP3(+), CD194(+)
Often lose CD7 expression
Cytotoxic markers (-)
• Clonal T-cell receptor gene rearrangement
• Complex chromosomal abnormalities; no one abnormality is characteristic of ATLL
Top Differential Diagnoses
• Mycosis fungoides
Similar clinical picture with epidermotropism & peripheral blood lymphocytosis
Also CD4(+), CD8(-) T cells, but CD25(-), FOXP3(-), & CD30(-)
• Anaplastic large cell lymphoma
FOXP3(-), CD194(-); ALK1 & EMA(+/-), unlike ATLL
Clinical Photograph of Adult T-Cell Leukemia/Lymphoma This clinical photograph shows an ulcerating lesion , which is 2.5 cm in the greatest dimension, from the foot of a person from the Caribbean region who was human T-cell leukemia virus type I (HTLV-I) (+).
Epithelial Involvement in Adult T-Cell Leukemia/Lymphoma This adult T-cell leukemia/lymphoma (ATLL) involves the mucosal epithelium. Note the small lymphocytes with irregular hyperchromatic nuclei infiltrating the squamous mucosa, forming Pautrier-like microabscesses . (Courtesy C. Bueso-Ramos, MD.)
Adult T-Cell Leukemia/Lymphoma at High Magnification High magnification of ATLL shows a population of medium-sized, atypical, and pleomorphic-appearing cells with hyperchromasia, atypical nuclear contours, focally prominent nucleoli, and vesicular chromatin. Mitotic figures are also seen.
Lack of *ALK* Gene Rearrangements This is a break-apart FISH test for the ALK gene, which shows fused (yellow) signals. This indicates that the lesion does not have ALK gene rearrangements. Unlike systemic anaplastic large cell lymphoma, ATLL does not show ALK gene rearrangements.
TERMINOLOGY
Abbreviations
• Adult T-cell leukemia/lymphoma (ATLL)
Synonyms
• Adult T-cell leukemia
Definitions
• T-cell lymphoma/leukemia of regulatory T cells [CD4(+), CD25(+), FOXP3(+)] caused by human T-cell leukemia virus type I (HTLV-I)
ETIOLOGY/PATHOGENESIS
Infectious Agents
• HTLV-I
Type C retrovirus, composed of single-stranded RNA, which is converted into double-strand DNA during infection
Virus is monoclonally integrated into host genome
Progresses to leukemia/lymphoma in < 5% of infected individuals
Long latency period
– Most exposed as infants/children
– Tumor often develops after 20 years of viral exposure
Transmitted through blood, sexual intercourse, or breast milk
HLA alleles A26, B4002, B4006, & B4801 may be predisposed to developing ATLL
Inflammatory diseases related to HTLV-I include tropical spastic paraparesis, HTLV-I-associated myelopathy, HTLV-I-associated uveitis, & infective dermatitis
Encodes tax (viral oncoprotein)
– Plays role in development of ATLL
– Activates transcription factors for T-cell proliferation genes
CLINICAL ISSUES
Epidemiology
• Age
Adults; most commonly in 6th or 7th decades
• Sex
M:F = 1.5:1.0
• Ethnicity
Endemic to Southwest Japan, Caribbean, South America, Australia, & Central Africa
Presentation
• Skin lesions
Develop in 50% of ATLL patients
Usually multiple nodules/tumors, papules, plaques, or macules
– Papules may cover large segments of body
Rarely, erythroderma, purpura, prurigo, or erythema multiforme
• Other sites of disease include lymph nodes, peripheral blood, bone, spleen & sometimes lung, liver, & CNS
Most patients have generalized lymphadenopathy
Hypercalcemia from increased osteoclast bone resorption







 , which is 2.5 cm in the greatest dimension, from the foot of a person from the Caribbean region who was human T-cell leukemia virus type I (HTLV-I) (+).
, which is 2.5 cm in the greatest dimension, from the foot of a person from the Caribbean region who was human T-cell leukemia virus type I (HTLV-I) (+).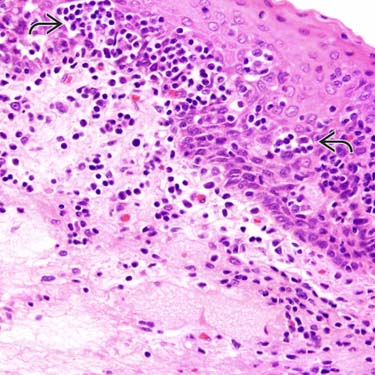
 . (Courtesy C. Bueso-Ramos, MD.)
. (Courtesy C. Bueso-Ramos, MD.)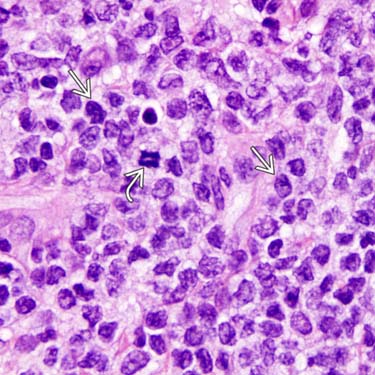
 with hyperchromasia, atypical nuclear contours, focally prominent nucleoli, and vesicular chromatin. Mitotic figures
with hyperchromasia, atypical nuclear contours, focally prominent nucleoli, and vesicular chromatin. Mitotic figures  are also seen.
are also seen.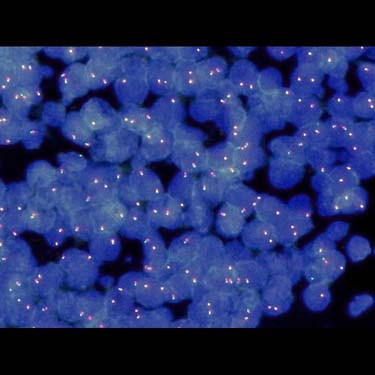
















 Acute subtype
Acute subtype







