and  blockers differ markedly in their effects and clinical applications, these drugs are considered separately in the following discussion.
blockers differ markedly in their effects and clinical applications, these drugs are considered separately in the following discussion.
High-Yield Terms to Learn
Competitive blocker A surmountable antagonist (eg, phentolamine); one that can be overcome by increasing the dose of agonist Epinephrine reversal Conversion of the pressor response to epinephrine (typical of large doses) to a blood pressure-lowering effect; caused by  blockers Intrinsic sympathomimetic activity (ISA) Partial agonist action by adrenoceptor blockers; typical of several
blockers Intrinsic sympathomimetic activity (ISA) Partial agonist action by adrenoceptor blockers; typical of several  blockers (eg, pindolol, acebutolol) Irreversible blocker A nonsurmountable inhibitor, usually because of covalent bond formation (eg, phenoxybenzamine) Membrane stabilizing activity (MSA) Local anesthetic action; typical of several
blockers (eg, pindolol, acebutolol) Irreversible blocker A nonsurmountable inhibitor, usually because of covalent bond formation (eg, phenoxybenzamine) Membrane stabilizing activity (MSA) Local anesthetic action; typical of several  blockers (eg, propranolol) Orthostatic hypotension Hypotension that is most marked in the upright position; caused by venous pooling (typical of
blockers (eg, propranolol) Orthostatic hypotension Hypotension that is most marked in the upright position; caused by venous pooling (typical of  blockade) or inadequate blood volume (caused by blood loss or excessive diuresis) Partial agonist A drug (eg, pindolol) that produces a smaller maximal effect than a full agonist and therefore can inhibit the effect of a full agonist Pheochromocytoma A tumor consisting of cells that release varying amounts of norepinephrine and epinephrine into the circulation
blockade) or inadequate blood volume (caused by blood loss or excessive diuresis) Partial agonist A drug (eg, pindolol) that produces a smaller maximal effect than a full agonist and therefore can inhibit the effect of a full agonist Pheochromocytoma A tumor consisting of cells that release varying amounts of norepinephrine and epinephrine into the circulation
Alpha-Blocking Drugs
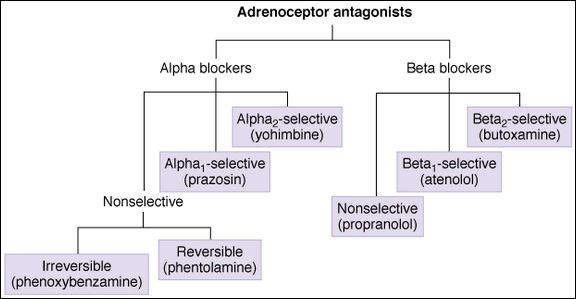
Classification
Subdivisions of the  blockers are based on selective affinity for
blockers are based on selective affinity for  1 versus
1 versus  2 receptors or a lack thereof. Other features used to classify the
2 receptors or a lack thereof. Other features used to classify the  -blocking drugs are their reversibility and duration of action.
-blocking drugs are their reversibility and duration of action.
Irreversible, Long-Acting
Phenoxybenzamine is the prototypical long-acting, irreversible  blocker. It is only slightly
blocker. It is only slightly  1 selective.
1 selective.
Reversible, Shorter-Acting
Phentolamine is a competitive, reversible blocking agent that does not distinguish between  1 and
1 and  2 receptors.
2 receptors.
Alpha1-Selective
Prazosin is a highly selective, reversible pharmacologic  1 blocker. Doxazosin, terazosin, and tamsulosin are similar drugs. The advantage of
1 blocker. Doxazosin, terazosin, and tamsulosin are similar drugs. The advantage of  1 selectivity is discussed in the following text.
1 selectivity is discussed in the following text.
Alpha2-Selective
Yohimbine and rauwolscine are  2-selective competitive pharmacologic antagonists. They are used primarily in research applications.
2-selective competitive pharmacologic antagonists. They are used primarily in research applications.
Pharmacokinetics
Alpha-blocking drugs are all active by the oral as well as the parenteral route, although phentolamine is rarely given orally. Phenoxybenzamine has a short elimination half-life but a long duration of action—about 48 h—because it binds covalently to its receptor. Phentolamine has a duration of action of 2-4 h when used orally and 20-40 min when given parenterally. Prazosin and the other  1-selective blockers act for 8-24 h.
1-selective blockers act for 8-24 h.
Mechanism of Action
Phenoxybenzamine binds covalently to the  receptor, thereby producing an irreversible (insurmountable) blockade. The other agents are competitive pharmacologic antagonists—that is, their effects can be surmounted by increased concentrations of agonist. This difference may be important in the treatment of pheochromocytoma because a massive release of catecholamines from the tumor may overcome a reversible blockade.
receptor, thereby producing an irreversible (insurmountable) blockade. The other agents are competitive pharmacologic antagonists—that is, their effects can be surmounted by increased concentrations of agonist. This difference may be important in the treatment of pheochromocytoma because a massive release of catecholamines from the tumor may overcome a reversible blockade.
Effects
Nonselective Blockers
These agents cause a predictable blockade of  -mediated responses to sympathetic nervous system discharge and exogenous sympathomimetics (ie, the
-mediated responses to sympathetic nervous system discharge and exogenous sympathomimetics (ie, the  responses listed in Table 9-1). The most important effects of nonselective
responses listed in Table 9-1). The most important effects of nonselective  blockers are those on the cardiovascular system: a reduction in vascular tone with a reduction of both arterial and venous pressures. There are no significant direct cardiac effects. However, the nonselective
blockers are those on the cardiovascular system: a reduction in vascular tone with a reduction of both arterial and venous pressures. There are no significant direct cardiac effects. However, the nonselective  blockers do cause baroreceptor reflex-mediated tachycardia as a result of the drop in mean arterial pressure (see Figure 6-4). This tachycardia may be exaggerated because the
blockers do cause baroreceptor reflex-mediated tachycardia as a result of the drop in mean arterial pressure (see Figure 6-4). This tachycardia may be exaggerated because the  2 receptors on adrenergic nerve terminals in the heart, which normally reduce the net release of norepinephrine, are also blocked (see Figure 6-3).
2 receptors on adrenergic nerve terminals in the heart, which normally reduce the net release of norepinephrine, are also blocked (see Figure 6-3).
Epinephrine reversal (Figure 10-1) is a predictable result of the use of this agonist in a patient who has received an  blocker. The term refers to a reversal in the blood pressure effect of large doses of epinephrine, from a pressor response (mediated by
blocker. The term refers to a reversal in the blood pressure effect of large doses of epinephrine, from a pressor response (mediated by  receptors) to a depressor response (mediated by
receptors) to a depressor response (mediated by  2 receptors). The effect is not observed with phenylephrine or norepinephrine because these drugs lack sufficient
2 receptors). The effect is not observed with phenylephrine or norepinephrine because these drugs lack sufficient  2 effects. Epinephrine reversal is occasionally seen as an unexpected (but predictable) effect of drugs for which
2 effects. Epinephrine reversal is occasionally seen as an unexpected (but predictable) effect of drugs for which  blockade is an adverse effect (eg, some phenothiazine tranquilizers, antihistamines).
blockade is an adverse effect (eg, some phenothiazine tranquilizers, antihistamines).
FIGURE 10-1
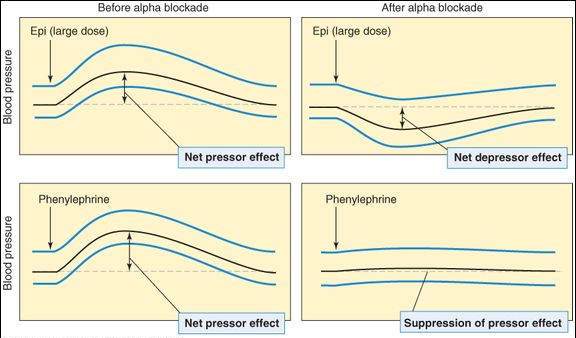
The effects of an  blocker, for example, phentolamine, on the blood pressure responses to epinephrine (epi) and phenylephrine. The epinephrine response exhibits reversal of the mean blood pressure change from a net increase (the
blocker, for example, phentolamine, on the blood pressure responses to epinephrine (epi) and phenylephrine. The epinephrine response exhibits reversal of the mean blood pressure change from a net increase (the  response) to a net decrease (the
response) to a net decrease (the  2 response). The response to phenylephrine is suppressed but not reversed, because phenylephrine is a “pure”
2 response). The response to phenylephrine is suppressed but not reversed, because phenylephrine is a “pure”  agonist without
agonist without  action.
action.
Selective  Blockers
Blockers
Because prazosin and its analogs block vascular  1 receptors much more effectively than the
1 receptors much more effectively than the  2-modulatory receptors associated with cardiac sympathetic nerve endings, these drugs cause much less reflex tachycardia than the nonselective
2-modulatory receptors associated with cardiac sympathetic nerve endings, these drugs cause much less reflex tachycardia than the nonselective  blockers when reducing blood pressure. These drugs also have important effects on smooth muscle in the prostate.
blockers when reducing blood pressure. These drugs also have important effects on smooth muscle in the prostate.
Clinical Uses
Nonselective  Blockers
Blockers
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


