Only a few cases have metastasized, usually to lymph nodes and lungs
Macroscopic
• Usually a few centimeters, can be up to 8 cm
Microscopic
• Composed of infiltrative lobules, islands, and cords of basaloid cells
Numerous cystic and ductular spaces with prominent cribriform pattern
• Cells are typically small, relatively monomorphic appearing, and cuboidal shaped
Ancillary Tests
• Epithelial cells stain positive with EMA, CEA-m, and cytokeratins (low and high molecular weight keratins)
• S100, p63, GFAP, SMA, MSA, and calponin often stain peripheral cells, consistent with myoepithelial differentiation
Top Differential Diagnoses
• Basal cell carcinoma (BCC)
• Metastatic adenoid cystic carcinoma
• Other primary cutaneous adnexal tumors
Adenoid Cystic Carcinoma Adenoid cystic carcinoma (ACC) at low magnification shows a dermal-based basaloid neoplasm with numerous cribriform spaces containing basophilic mucin and showing a prominent Swiss cheese-like pattern.
Adenoid Cystic Carcinoma With Prominent Mucin Higher magnification of ACC shows relatively bland basaloid cells surrounding the ductal lumina containing prominent collections of blue mucinous material.
Adenoid Cystic Carcinoma With Perineural Invasion ACC frequently shows perineural invasion, which accounts for its high local recurrence rate. Here, a large central nerve is surrounded by multiple tumor cords and ducts.
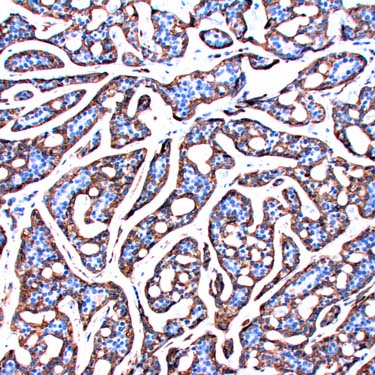
SMA Immunohistochemistry in ACC ACC typically demonstrates expression of myoepithelial markers including SMA (shown here), MSA, calponin, cytokeratins, S100, and GFAP.

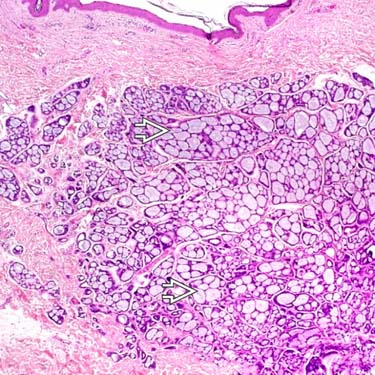
 containing basophilic mucin and showing a prominent Swiss cheese-like pattern.
containing basophilic mucin and showing a prominent Swiss cheese-like pattern.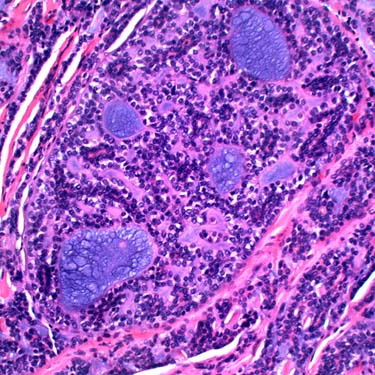
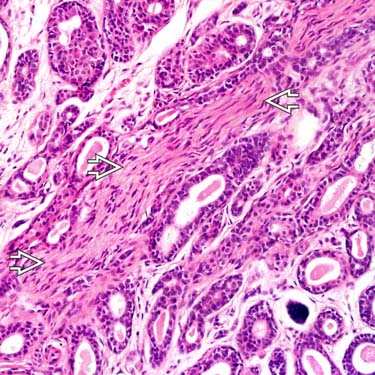
 is surrounded by multiple tumor cords and ducts.
is surrounded by multiple tumor cords and ducts.