• Most often occurs in India, Chile, Pakistan, and Ecuador
Females more often affected
• Symptoms often vague, nonspecific
Often incidental finding at cholecystectomy for cholecystitis or cholelithiasis
• Surgery is most effective and only potentially curative treatment
Tumor stage probably most important prognostic factor
• Overall 5-year survival ∼ 10%
Macroscopic
• Area of thickening and induration of gallbladder wall
Tumor may be difficult to appreciate grossly
• Exophytic or polypoid mucosal mass
Microscopic
• Malignant glands, clusters, or individual cells invading gallbladder wall
Some extremely well-differentiated tumors are deceptively bland and difficult to recognize
Multiple histologic variants recognized by WHO
• Majority of cases associated with epithelial dysplasia &/or carcinoma in situ
Gallbladder Adenocarcinoma, Gross This gross cholecystectomy specimen with adenocarcinoma contains areas of mucosal irregularity associated with thickening of the gallbladder wall .
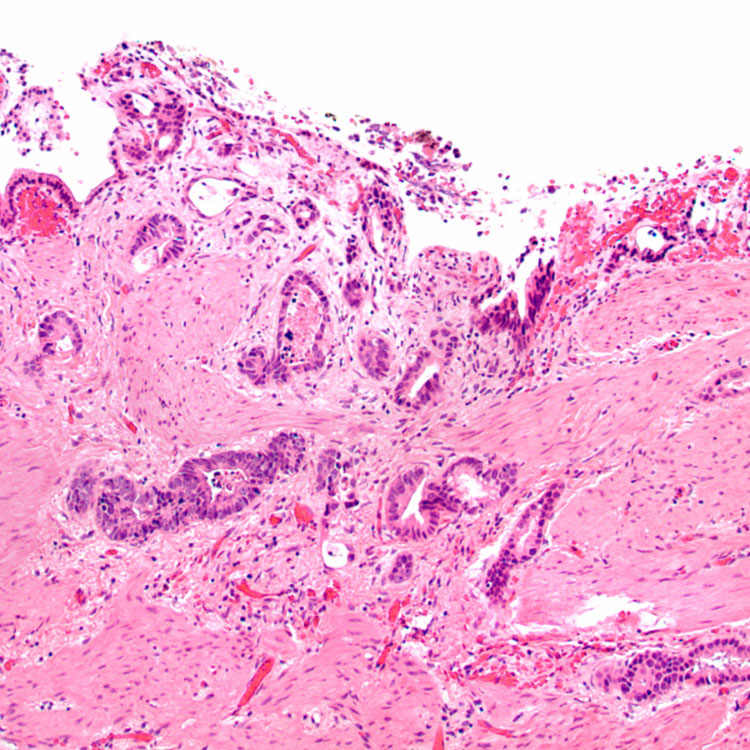
Gallbladder Adenocarcinoma, Low Power This low-power view of gallbladder adenocarcinoma shows irregular neoplastic glands invading the smooth muscle of the gallbladder wall.
Gallbladder Adenocarcinoma, Perineural Invasion Perineural invasion is frequently seen in association with gallbladder adenocarcinoma.
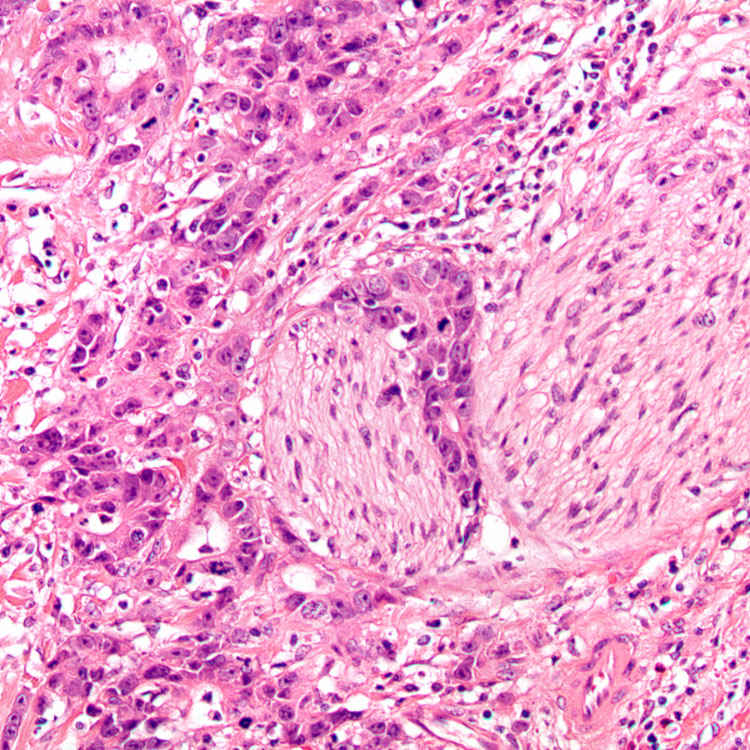
Gallbladder Adenocarcinoma, Desmoplasia Irregular, abortive glands and single cells have associated prominent desmoplastic stroma in this invasive gallbladder adenocarcinoma.
TERMINOLOGY
Definitions
• Malignant glandular epithelial neoplasm of gallbladder
ETIOLOGY/PATHOGENESIS
Risk Factors
• Chronic inflammation
Chronic cholecystitis and cholelithiasis
– > 80% of gallbladder adenocarcinomas are associated with gallstones
Chronic biliary infections
– Opisthorchis viverrini
– Salmonella typhi
Pancreatobiliary reflux
• Porcelain gallbladder
> 10% of affected patients have or will develop adenocarcinoma
• Primary sclerosing cholangitis (PSC)
Gallbladder adenocarcinoma reported in ∼ 14% of patients undergoing liver transplantation for PSC
• Gastrointestinal polyposis
Familial adenomatous polyposis coli
Gardner syndrome
Peutz-Jeghers syndrome
Molecular Alterations
• Reported KRAS mutation rates vary from 0-50%
• TP53 mutations common in late-stage disease
CLINICAL ISSUES
Epidemiology
• Incidence
Reported 1.43 cases per 100,000 persons at risk
Rates of incidental diagnosis at time of laparoscopic cholecystectomy range from 0.28-2.10%
• Age
Predominantly affects elderly patients
Mean: 65 years
• Sex
Females more often affected (F:M = 3:1)
• Ethnicity
Most often occurs in India, Chile, Pakistan, and Ecuador
In western countries, Latin American and Native American individuals at greatest risk
Presentation
• Symptoms often vague, nonspecific
Upper abdominal pain
Weight loss
Only gold members can continue reading. Log In or Register to continue









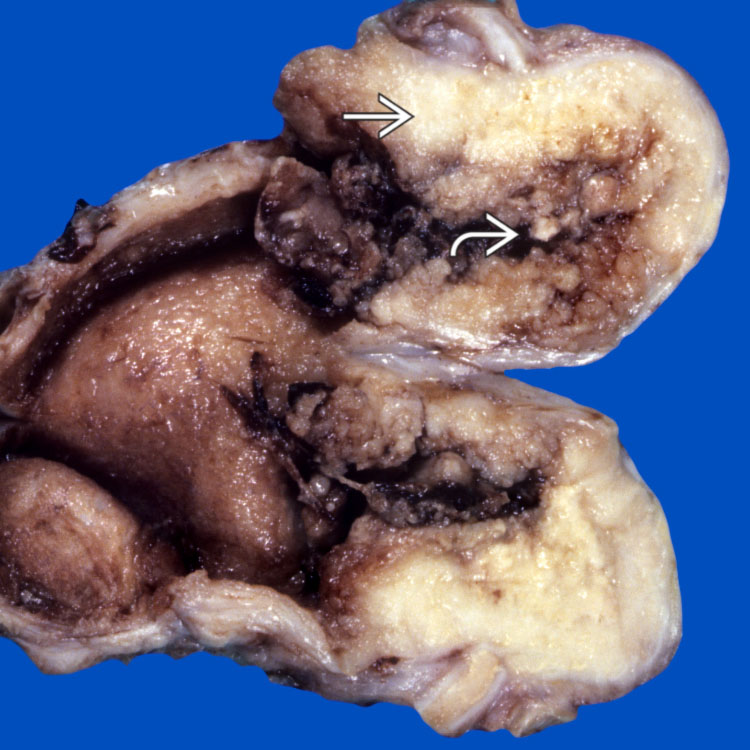
 associated with thickening of the gallbladder wall
associated with thickening of the gallbladder wall  .
.