Patient’s Story
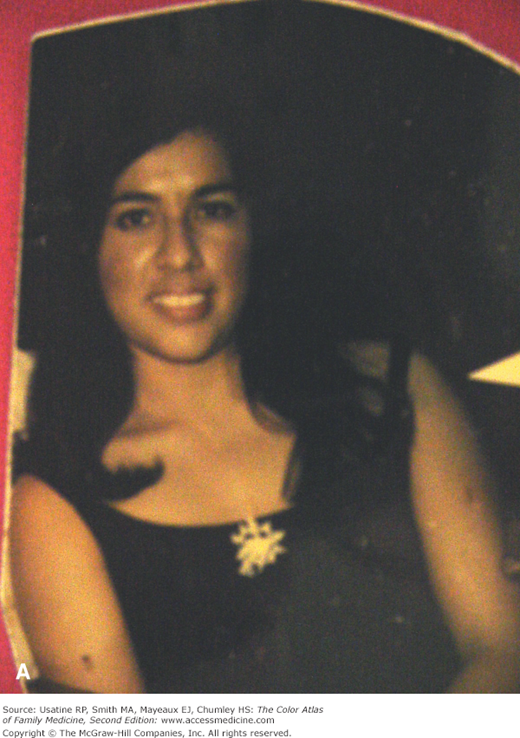
A 60-year-old man presents to his family physician with severe headache and weakness (Figure 228-1). He also noted enlargement of his hands (Figure 228-2), which made him remove his wedding ring when it became too tight, and feet (his shoe size had increased). He said his voice seemed to be deeper and his hands feel doughy and sweaty. Laboratory testing reveals an elevated insulin-like growth factor (IGF)-I, and there is a failure of growth hormone (GH) suppression following an oral glucose load confirming the diagnosis of acromegaly. Computed tomography (CT) scan of the head demonstrates a pituitary adenoma.
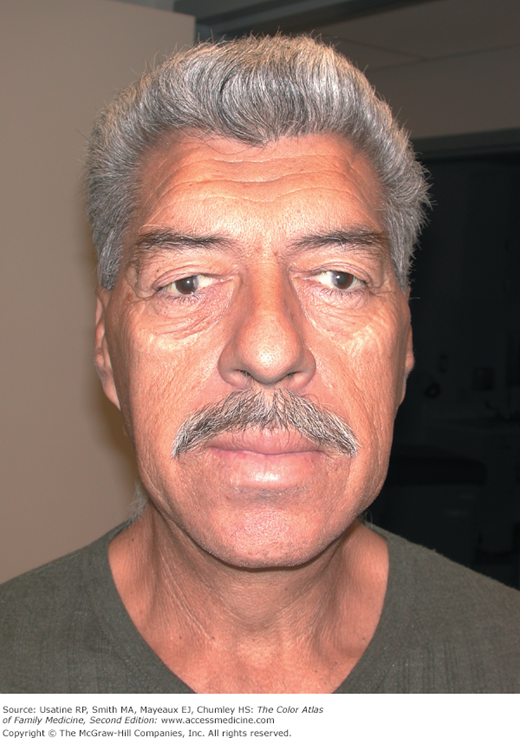
Figure 228-2
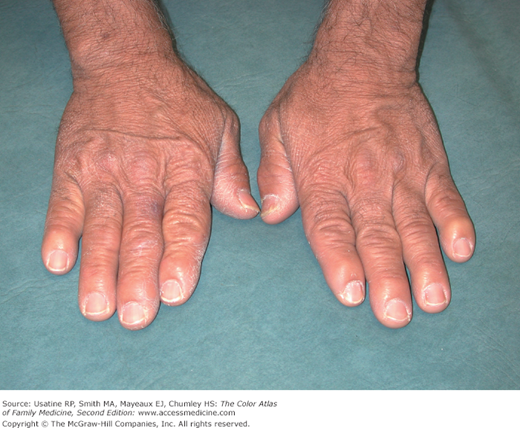
The man in Figure 228-1 with acromegaly producing hands that are large and doughy with widened fingers. (Courtesy of Richard P. Usatine, MD.)
Introduction
Epidemiology
- Rare (5/1,000,000 adults)1
- Most typically caused by a pituitary somatotrope macroadenoma. It may also be caused by growth hormone-releasing hormone (GHRH) excess from lesions of the pancreas, lung, or ovaries, or from a chest or abdominal carcinoid tumor.
- The disorder is usually sporadic, but may be familial (<5%) and has been associated with other endocrine tumors (e.g., multiple endocrine neoplasia type I).1
- In a Spanish multicenter epidemiologic study, the reported mean age at diagnosis was 45 years.2
- The occurrence of GH hypersecretion in children and adolescents, prior to epiphyseal closure, causes gigantism.
Etiology and Pathophysiology
- The clinical signs and symptoms of acromegaly result from GH excess that stimulates linear and organ growth (through IGF-I), soft-tissue swelling, and chondrocyte action.
- Acromegaly is also associated with insulin resistance and an increased risk of cardiovascular disease; the latter appears to be a result of pressure-related arterial and left ventricular stiffening rather than atherosclerotic disease.3
- An increased risk for several cancers among these patients may be a result of the proliferative and antiapoptotic activity associated with increased circulating levels of IGF-I.
Diagnosis
The diagnosis of acromegaly is established by documenting autonomous GH hypersecretion and by pituitary imaging.
The clinical manifestations of acromegaly are often subtle and may not be noticed for many years. Gigantism occurs if excessive GH exposure occurs before closure of the epiphyses; acromegaly develops after closure of the epiphyses. Clinical features of acromegaly include1:
- Soft-tissue swelling resulting in hand and foot enlargement (Figure 228-2).
- Kyphoscoliosis and skeletal hyperostosis.
- Coarse facial features and a large fleshy nose (Figures 228-1 and 228-3).
- Frontal bossing.
- Jaw malocclusion and overbite.
- Hyperhidrosis and oily skin.
- Other common features are deep voice (soft-tissue swelling of vocal cords), arthropathy, carpel tunnel syndrome, kyphosis, proximal muscle weakness, and fatigue; patients may complain of headache and visual field defects (expanding tumor), paresthesias, and sexual dysfunction.1
- Associated medical conditions include sleep apnea (60%), coronary heart disease (20% to 90% depending on duration and associated hypertension), and diabetes mellitus (25%). There also appears to be an increase in intracranial aneurysms.4
- In one study (N = 55), approximately two-thirds of women had anovulatory cycles; some believed related to elevated hormone levels.5