Minority of patients have associated lipase hypersecretion paraneoplastic syndrome
Macroscopic
• Solid, well-circumscribed, fleshy mass
• Average 10 cm in diameter (range: 2-30 cm)
Microscopic
• Densely cellular with multiple architectural patterns, most commonly acinar or solid
• Uniform nuclei with central prominent nucleolus
Eosinophilic, finely granular cytoplasm
• Minimal to moderate finely granular, eosinophilic to amphophilic cytoplasm
• Typically have minimal stroma
Ancillary Tests
• Immunohistochemistry
Pancreatic exocrine enzymes: Trypsin (97%), chymotrypsin (66-95%), and lipase (70-84%)
Cytokeratin 8 and 18
Focal staining for synaptophysin or chromogranin (35-54%), which may cause confusion with neuroendocrine neoplasms
• PAS positive, resistant to diastase digestion
Many have insufficient quantities of zymogen granules, resulting in negative stain
• Genetic alterations
Alterations in APC/β-catenin pathway (24% of ACC)
Allelic loss of chromosome arm 11p (50% of ACC)
Gross Specimen This relatively well-circumscribed acinar cell carcinoma (ACC) is large, fleshy, and white-tan with a lobular configuration and easily identifiable necrosis.
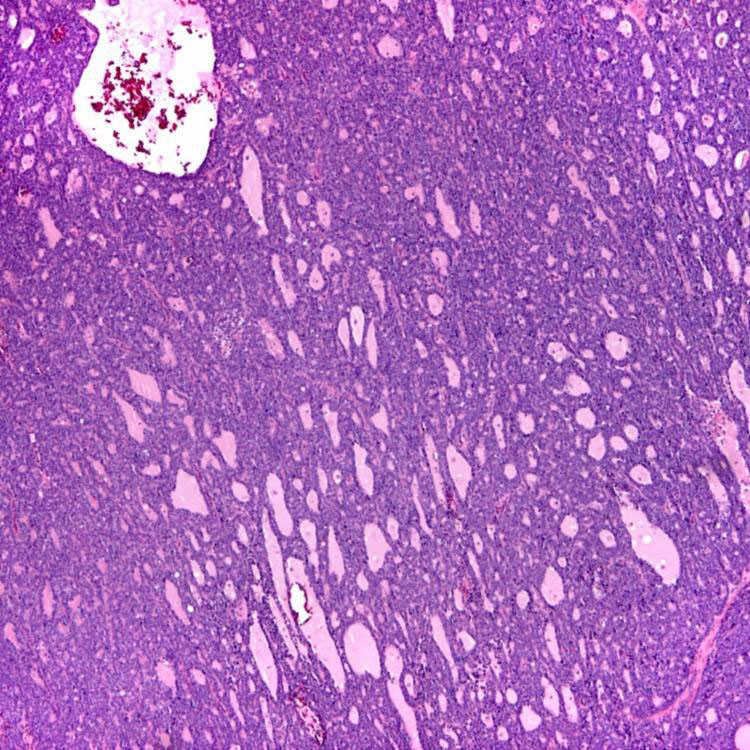
Acinar and Glandular Patterns With Minimal Stroma At low power, ACCs are densely cellular and typically have a relatively small or no significant stromal component. Note the well-formed acinar and glandular patterns.
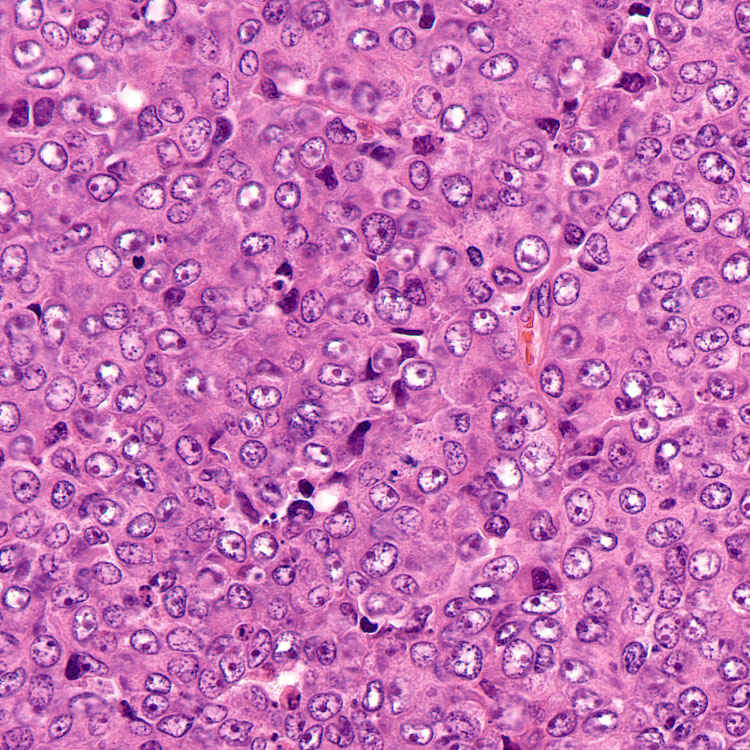
Nuclear Features This ACC with a solid growth pattern shows solid sheets of neoplastic cells with relatively uniform nuclei featuring vesicular chromatin, characteristic prominent nucleoli, and eosinophilic cytoplasm.
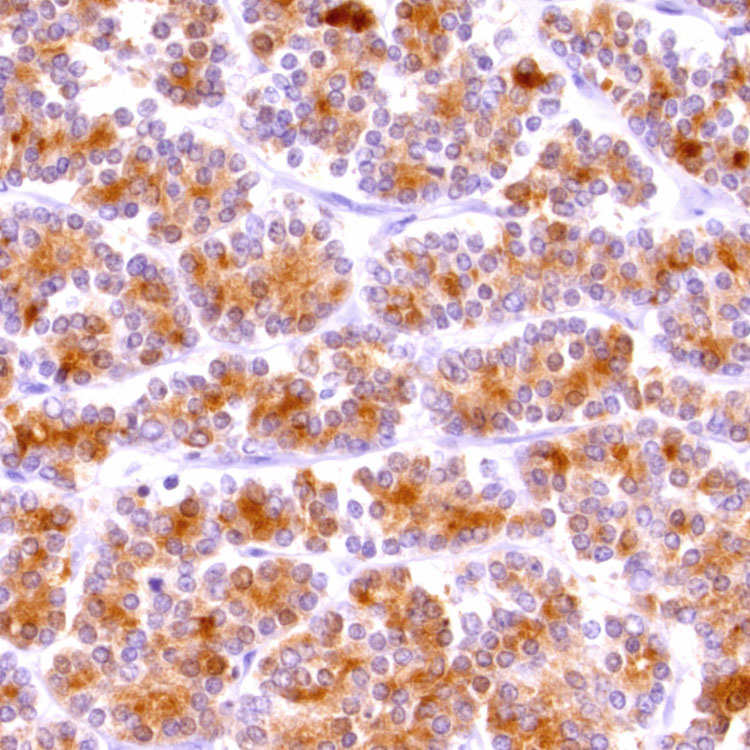
Acinar Cell Carcinoma, Immunohistochemistry Antibodies against pancreatic exocrine enzymes are the most sensitive marker of ACC. Note the cytoplasmic staining for trypsin. Chymotrypsin can be equally beneficial, and lipase is detected slightly less often.
TERMINOLOGY
Abbreviations
• Acinar cell carcinoma (ACC)
Definitions
• Malignant exocrine carcinoma with acinar differentiation
Produces pancreatic exocrine enzymes in zymogen granules
CLINICAL ISSUES
Epidemiology
• Incidence
1-2% of primary pancreatic neoplasms
• Age
Between 5th and 7th decades of life (mean: 58 years)