Anterior abdominal wall105
Introduction
Abdominal walls
11.1. Anterior abdominal wall
Surface anatomy and regions
Superficial and deep fascia
Clinical examination
In the midline, from top to bottom
Right and left, from top to bottom
Quadrants
Muscles of anterior abdominal wall (Fig. 11.2)
Rectus abdominis muscle
Sheet muscles: external and internal obliques, transversus abdominis
Rectus sheath
Action of the muscles as a whole
Nerve supply of anterior abdominal wall (Fig. 11.2)
Blood supply and lymph drainage of anterior abdominal wall
Arteries
Veins
Lymph
Abdominal incisions
11.2. Inguinal canal, scrotum, testis, inguinal hernias (Figs 11.4, 11.5)
The inguinal canal
Deep (internal) inguinal ring
Superficial (external) inguinal ring
Inguinal canal – the pathway between the two rings (Figs 11.4, 11.5)
Spermatic cord
Ilioinguinal nerve L1
Scrotum (Fig. 11.6)
Testis (Fig. 11.6)
Testicular descent
Retractile testes
Testicular malignancy and lymph drainage
Testicular torsion
Vasectomy
Swellings arising in the testis
Inguinal hernias (Fig. 11.7)
Types of inguinal hernia
Is it an inguinal hernia or a scrotal swelling?
Inguinal region in the female
11.3. Arrangement of the gut tube in the abdominal cavity
Some embryological considerations
In the peritoneal cavity…
Names – caution!
Parts of the peritoneal cavity
Pouches and disease
11.4. Great vessels of the abdomen, sympathetic chain
Aorta
Branches of the aorta (Fig. 11.11)
Inferior vena cava (Fig. 11.12)
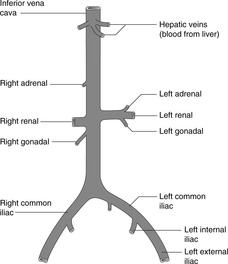
Fig. 11.12
Sympathetic chain
11.5. Foregut and associated structures: pancreas, spleen, liver, gall bladder
Oesophagus
Hiatus hernia
Stomach (Figs 11.13, 11.14)
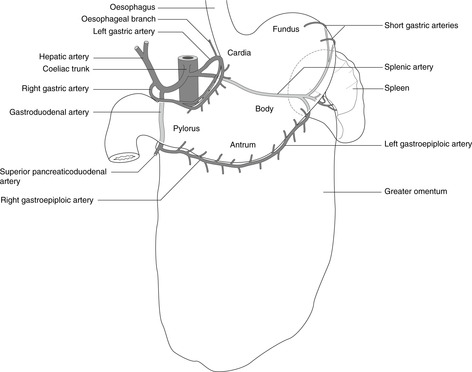
Fig. 11.13
Radiology of the stomach (Fig. 11.14)
Lesser omentum and lesser sac (Fig. 11.15)
Greater omentum, gastrosplenic ligament and splenorenal (lienorenal) ligament (Fig. 11.15)
Duodenum (Fig. 11.16)
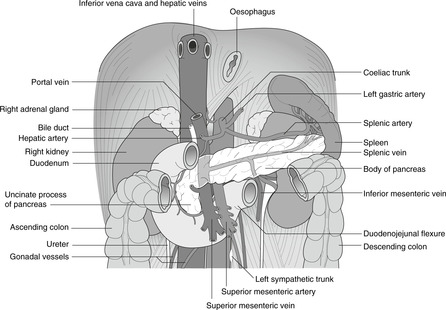
Fig. 11.16
Pancreas (Fig. 11.16)
Duct system (Figs 11.16, 11.17)
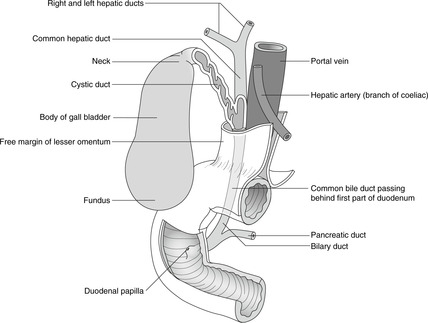
Fig. 11.17
Blood supply
Pancreatic disease
Spleen (Fig. 11.16)
Splenic injury and disease
Liver and biliary system (Fig. 11.18, Fig. 11.19, Fig. 11.20 and Fig. 11.21)
Position and surface anatomy
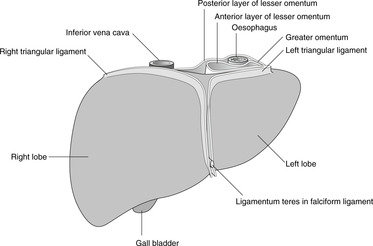
Fig. 11.18
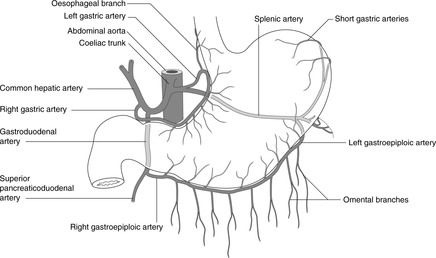
Fig. 11.21
Diaphragmatic and peritoneal attachments of the liver, bare area
Parts of the liver
Inferior vena cava and the liver
Biliary tree and gall bladder (Fig. 11.17)
Biliary obstruction, obstructive jaundice (Fig. 11.20)
Blood supply of foregut derivatives: oesophagus, stomach, proximal duodenum, liver, gall bladder, pancreas, spleen – coeliac artery (Fig. 11.21)
Boundaries of the epiploic foramen (of Winslow)
Bleeding from the liver, Pringle’s manoeuvre
Lymph drainage of foregut: stomach, liver, spleen, pancreas, duodenum, Virchow’s node
11.6. Midgut and hindgut
Midgut
Small bowel: jejunum and ileum

Abdomen, pelvis and perineum
11.2 Inguinal canal, scrotum, testis, inguinal hernias109
11.3 Arrangement of the gut tube in the abdominal cavity113
11.4 Great vessels of the abdomen, sympathetic chain116
11.5 Foregut and associated structures: pancreas, spleen, liver, gall bladder118
11.6 Midgut and hindgut126
11.7 Portal venous system: venous drainage of the gut tube and associated organs129
11.8 Nerve supply of the gut tube, gut pain131
11.9 Posterior abdominal wall, diaphragm and associated structures132
11.10 Kidneys, ureters, adrenals134
11.11 Pelvis136
11.12 Perineum145
11.13 Autonomic nervous system in the abdomen and pelvis: a review151
11.14 Summary of surface markings and vertebral levels152
The abdominal or peritoneal cavity is separated from the thorax by the diaphragm, and from the perineum below by the pelvic diaphragm or levator ani muscle. It is supported by the vertebral column, rib cage, and the bony pelvis formed by the two hip bones and the sacrum. Upper abdominal organs (e.g. liver, stomach, spleen, kidneys) are to some extent protected by the rib cage, while others low down (e.g. bladder, uterus, prostate) are protected by the bony pelvis. It follows from this that organs most closely related to bone may be damaged by injuries to these bones: for example fractures of the left tenth rib may damage the spleen.
The abdominal walls between rib cage and bony pelvis are formed by muscles and fascia. Details of the posterior abdominal wall are of no great clinical importance, and they are considered only briefly in section 11.9. The anterior abdominal wall, on the other hand, being so often inspected, palpated and incised, needs a section of its own.
The anterior abdominal wall is divided into nine regions or four quadrants. The regions are in the midline from top to bottom, epigastrium, umbilical and hypogastrium, and the lateral regions are, from top to bottom, hypochondrial, lumbar and iliac fossa or inguinal. The quadrants are right upper, right lower, left upper and left lower. Muscles of the abdominal wall are external oblique, internal oblique, transversus abdominis and rectus abdominis. The blood supply and innervation of the anterior abdominal wall are relevant to trauma, disease and surgery.
You should:
• list the nine regions and four quadrants and the principal organs and structures that lie deep to them and which can be palpated in those regions
• describe the muscular components of the anterior abdominal wall
• describe the blood supply and innervation of the anterior abdominal wall.
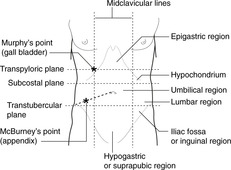
The nine descriptive regions of the anterior abdominal wall (Fig. 11.1) are demarcated by two vertical and two horizontal planes. The vertical planes are the right and left midclavicular lines, and the horizontal planes the transpyloric (by most people, although some prefer the subcostal) and transtubercular planes.
• Transpyloric plane: vertebral level L1. This intersects the rib cage at the tip of the ninth costal cartilage. It is about halfway between the suprasternal notch and the pubic symphysis, or about halfway between the xiphoid process and the umbilicus, and it marks the position or level of several internal structures (e.g. pylorus, gall bladder, renal hila, origin of superior mesenteric artery).
• Subcostal plane: vertebral level L2/3. This is the plane marking the lowest point of the rib cage. In an ill, bedridden patient it can be difficult to find, particularly if the patient is obese.
• Transtubercular plane: vertebral level L3. The tubercles of the iliac crests are palpable some distance behind the anterior superior iliac spines (ASIS). In practice, the ASIS is easier to feel than the tubercles and the plane of the ASIS may be substituted for the transtubercular plane. In any case, these lines are only rough guides.
Between the skin and the muscles of the abdominal wall is the superficial (Camper’s) fascia: thin in a lean person, and thick in a fat person. The deep (Scarpas’s) fascia is a tough membrane on the external aspect of the muscles.
• Epigastrium. Stomach tumours may be palpable here, and pain from foregut structures (as far as the duodenal papilla) is usually referred to this area. The pulsating aorta is palpable slightly to the left of the midline.
• Umbilical region. Pain from midgut structures (duodenal papilla to splenic flexure of the colon) is usually referred to this area. The pulsating aorta is palpable above the umbilicus.
• Hypogastrium or suprapubic region. Enlarged pelvic organs may be palpable here (uterus, bladder) and pain from hindgut structures (descending colon to anal canal) is usually referred to this area.
• Hypochondriac region. On the right, the liver and the gall bladder may be palpable. The tip of the right ninth costal cartilage, the usual surface marking of the fundus of the gall bladder, is Murphy’s point. On the left an enlarged spleen (at least three times normal size) may be palpable.
• Lumbar region. The lower poles of the kidneys may be palpated here, and the descending colon may be palpable on the left.
• Iliac fossa or inguinal region. The usual surface marking of the base of the appendix is McBurney’s point: one-third of the way along a line from the right anterior superior iliac spine to the umbilicus. Tenderness in the right iliac fossa may signify disease of the appendix, and a hard mass here may be cancer of the caecum or ascending colon. The descending colon may be palpable on the left, and a mass in the left iliac fossa may signify a tumour of the sigmoid colon or bulky faeces.
Quadrants are also commonly used for description:
• right upper quadrant (gall bladder, liver)
• left upper quadrant (enlarged spleen)
• right lower quadrant (appendix, caecum)
• left lower quadrant (sigmoid colon).
• Rectus abdominis muscle which lies on either side of the midline.
• The sheet muscles: three anterolateral muscle sheets: external oblique, internal oblique and transversus abdominis muscles.
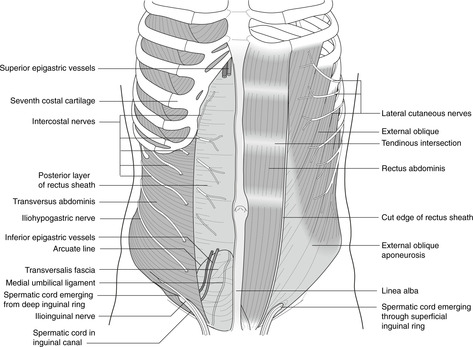
This runs from rib cage and sternum to the pubic bones. On contraction, it compresses the abdominal contents and is a flexor of the spinal column. Transverse tendinous intersections are (in a lean person) visible and palpable above the umbilicus. They are of little significance except that when cut they bleed profusely.
• Linea semilunaris. This is the lateral margin of the rectus abdominis. It meets the rib cage at or near the ninth costal cartilage (vertebral level L1, transpyloric plane). It can be made more obvious (to either hand or eye) by asking the supine patient to raise the head, causing rectus abdominis to contract.
• Linea alba. This is in the midline between the rectus muscles and is usually palpable as a slight depression. Weaknesses in the linea alba may result in midline herniation of abdominal contents, often at the umbilicus.
The sheet muscles are attached to lumbar fascia posteriorly (don’t bother with details), to the ribs and costal cartilages superiorly, to the hip bones inferiorly and the inguinal ligament (from ASIS to pubic tubercles) inferiorly. Medially, muscle fibres give way to broad, flat tendons (aponeuroses) which form the rectus sheath around the rectus abdominis muscle. Fibres of these muscles run in different directions, reinforcing each other, and inferiorly they form the inguinal canal through which the spermatic cord in the male, and the round ligament of the uterus in the female, pass from abdomen to scrotum or labia majora respectively. The inguinal canal is an important area (see section 11.2, below).
• External oblique muscle. From the lower eight ribs, fibres pass downwards and medially to the linea alba, pubic region and inguinal ligament, and inferiorly to the anterior superior iliac spine and iliac crest. The aponeurosis of external oblique contributes to the anterior wall of the rectus sheath. Along a line from the anterior superior iliac spine to the pubic tubercle, the aponeurosis is thickened to form the inguinal ligament, where the deep fascia of the thigh is attached to the external oblique aponeurosis.
• Internal oblique muscle. From the lateral part of the inguinal ligament, the iliac crest and the lumbar fascia, these fibres pass upwards and medially to the costal margin and the linea alba. The aponeurosis of internal oblique splits to contribute to both anterior and posterior walls of the rectus sheath (Fig. 11.3). The lowest fibres, arising from the inguinal ligament, arch down to attach medially with similar fibres of transversus abdominis to the pubic tubercle as the conjoint tendon (see section 11.2).
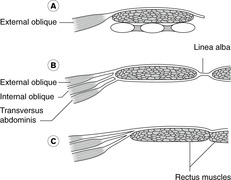
• Transversus abdominis muscle. From the six lowest ribs, lumbar fascia, iliac crest and the lateral part of the inguinal ligament, fibres run across to the linea alba contributing to the rectus sheath (Fig. 11.3). As with internal oblique, the lowest fibres arch down to attach to the pubic tubercle as the conjoint tendon.
• Transversalis fascia. This layer of connective tissue separates the muscles of the anterior abdominal wall from the parietal peritoneum.
The usual pattern is shown in Fig. 11.3, although there is considerable variation. Inferiorly, since the aponeuroses of all three sheet muscles pass anterior to rectus abdominis, the only tissue separating rectus abdominis from the parietal peritoneum is transversalis fascia. Above this on the posterior aspect of rectus abdominis is the arcuate line – the free lower extremity of that part of the rectus sheath that passes posterior to rectus abdominis.
The sheet muscles and rectus abdominis are active in trunk movements: flexion, lateral flexion and twisting. They compress the abdominal contents during defecation and provide support and stability during lifting. Asymmetrical spasm of these muscles during youth and adolescence has been implicated in cases of scoliosis (twisted spine).
This is from segmental nerves T7–L1. Intercostal nerves leave the costal grooves where the ribs turn superiorly, and continue into the abdominal wall. T12 segmental nerve is the subcostal nerve. L1 segmental nerve divides into two: the more cranial is the iliohypogastric, which principally supplies the abdominal wall, the more caudal the ilioinguinal, which is diverted to the anterior scrotum or labia majora, and the medial thigh.
Segmental nerves T7–12 travel in the abdominal wall between transversus abdominis and internal oblique, sending branches through these muscles to more superficial structures (e.g. skin) and internally to the peritoneum. The iliohypogastric and ilioinguinal nerves (L1) posteriorly are found between transversus and internal oblique, but in the region of the anterior superior iliac spine they penetrate internal oblique and run between internal and external obliques. This apparently trivial detail is relevant to inguinal anatomy and to incisions near McBurney’s point, for example for appendicectomy (see later).
• Sensory fibres in the nerves supply abdominal skin, wall and peritoneum (as well as thoracic skin and pleura). Cell bodies of sensory fibres are in the dorsal root ganglion of the appropriate nerve. See dermatome map (Fig. 6.6, p. 36). Note that the dermatome over the xiphoid process is (usually) T8, over the umbilicus T10, and over the pubic symphysis T12/L1.
• Motor fibres in the nerves supply the sheet muscles and the rectus abdominis. The cell bodies of the motor neurons are in the ventral horn of grey matter of the appropriate segment of the spinal cord.
• Intercostal arteries, part of the intercostal neurovascular bundles, approach from the lateral aspect.
• Epigastric arteries. Posterior to rectus abdominis muscle are:
– superior epigastric artery: a continuation of the internal thoracic artery from the subclavian
– inferior epigastric artery: a branch of the external iliac/femoral.
These freely anastomose and this may become a bypass channel for an aortic blockage (e.g. coarctation, see Fig. 10.25, p. 88).
• Branches of segmental lumbar arteries supply the posterior abdominal wall.
Intercostal veins drain to the azygos system. Lumbar (segmental) veins drain to the veins of the posterior abdominal wall and the azygos system (details not necessary), and the superior and inferior epigastric veins drain to subclavian and femoral veins respectively. Anastomoses between these venous channels may provide a bypass for a blockage of the inferior vena cava.
The lymph drainage of the anterior abdominal wall is roughly in quadrants: superiorly to right and left axillary nodes, and inferiorly to right and left inguinal nodes.
• Median incisions. The linea alba is a nerveless and comparatively bloodless plane.
• Paramedian incisions. Nerves enter rectus abdominis muscles from the lateral aspect, so in paramedian incisions, the anterior layer of the rectus sheath is incised and the rectus abdominis muscle displaced laterally so as not to tear the nerves. It is better to avoid incisions through the tendinous intersections, if possible: they bleed profusely.
• Incisions through the sheet muscles, e.g. a gridiron incision near McBurney’s point for appendicectomy. Muscle fibres need only be separated to give sufficient access, but it is worth noting that the L1 nerves (ilioinguinal and iliohypogastric) are in the vicinity of an incision over McBurney’s point, and that damage to the iliohypogastric nerve might weaken the muscles of the anterior abdominal wall in the inguinal region, increasing the possibility of a subsequent inguinal hernia.
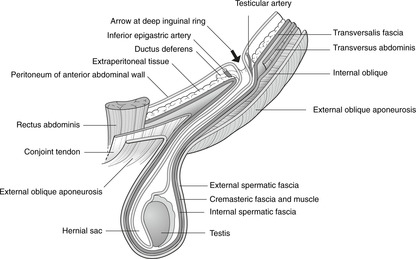
The inguinal canal is a weak spot in the anterior abdominal wall. In the male it transmits structures to and from the testis; in the female it is much smaller. The internal aspect of the canal is the deep inguinal ring; the external aspect is the superficial ring. In embryonic life the testis migrates from the abdomen to the scrotum. It is covered in the scrotum by three layers of fascia, and most intimately, by the tunica vaginalis, the cavity of which is a part of the peritoneal cavity that becomes detached during development. The abdominal origin of the testis is reflected in its vascular supply, and also its lymph drainage to para-aortic nodes, unlike that of scrotal skin to inguinal nodes.
Imagine the developing testis inside the abdomen trying to make its way out. It must first penetrate the transversalis fascia: the defect in this layer so caused is the:
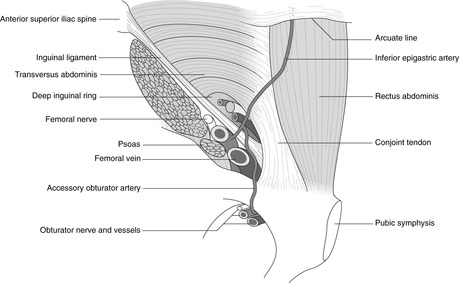
This is roughly circular and its surface marking is about 2cm above the femoral pulse at the inguinal ligament, the pulse being roughly halfway between the anterior superior iliac spine and the pubic tubercle. The deep ring is immediately lateral to the inferior epigastric artery passing up on the posterior surface of the rectus abdominis muscle.
Emerging from the deep inguinal ring, the testis makes its way downwards and medially, roughly parallel to and slightly above the inguinal ligament, through (in order) transversus abdominis and internal oblique to arrive at a defect in external oblique, the:
This is a triangular defect in external oblique, the base of which is medial to the pubic tubercle, and the apex of which points up and laterally so that most of the superficial ring is more-or-less directly above the pubic tubercle.
• The floor of the canal is formed by the inguinal ligament.
• The anterior wall is formed by external oblique aponeurosis throughout, reinforced laterally (over the deep ring) by internal oblique.
• The posterior wall is formed by transversalis fascia throughout, reinforced medially (deep to the superficial ring) by the conjoint tendon (united internal oblique and transversus abdominis) attached to the pubic tubercle.
• The roof of the canal is made up of the fibres of internal oblique arching over the contents of the inguinal canal to form the conjoint tendon.
In coughing, straining and lifting, the muscles of the anterior abdominal wall contract and the diaphragm is fixed so that abdominal contents (e.g. bowel) might be forced through the potential weak spot of the inguinal region. This is minimised by the way in which the muscles move when contracting which results in the arching fibres of internal oblique being pulled inferiorly to cover the anterior aspect of the deep inguinal ring, thereby reinforcing it and reducing the size of the potential weakness.
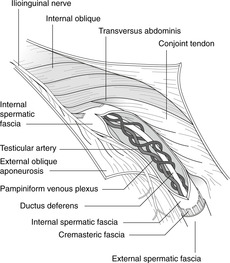
As the testis ‘pushes’ its way through the inguinal canal towards the scrotum, it drags with it the ductus deferens, arteries, veins and nerves passing to the testis. These structures constitute the spermatic cord, which acquires coverings that to some extent reflect the layers of the abdominal wall through which they have passed. From inside out these are:
• the internal spermatic fascia
• the cremasteric fascia and cremaster muscle
• the external spermatic fascia.
The spermatic cord also includes:
• the testicular artery, on each side a direct branch of the aorta
• the pampiniform plexus of veins which form the testicular vein draining on the right to the inferior vena cava and on the left to the renal vein
• testicular lymphatics passing to para-aortic nodes (the lymph drainage of the testis thus reflecting its arterial supply)
• the genital branch of the genitofemoral nerve (L1, 2) which supplies cremaster muscle with involuntary motor fibres – cremaster muscle retracts the testis
• sympathetic nerve fibres
• blood vessels serving the ductus deferens.
This supplies anterior scrotal and penile skin. It enters the inguinal canal not through the deep inguinal ring, but from the lateral aspect. In the region of the anterior superior iliac spine it lies between internal and external obliques, and so, as it runs down parallel to the inguinal ligament it is joined in the inguinal canal by the structures which have entered through the deep inguinal ring. The ilioinguinal nerve passes through the superficial inguinal ring on the surface of the spermatic cord.
The scrotum is equivalent to the labia majora in the female. It is a body wall structure, so:
• its arterial supply is from body wall arteries (pudendal, femoral)
• its venous drainage is to body wall veins (pudendal, great saphenous)
• its lymph drainage is mainly to inguinal lymph nodes (very important)
• its cutaneous sensory nerve supply is from ilioinguinal (L1), genital branch of genitofemoral (L1, 2) and scrotal branches of the pudendal (S2, 3, 4) nerves.
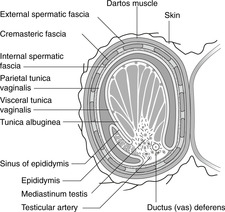
Scrotal skin is thin and contains smooth muscle fibres – dartos, supplied by sympathetic fibres, which contract in the cold to cause wrinkling.
In the scrotum, each testis is invaginated into its serous membrane, the tunica vaginalis, much as the lung is invaginated into the pleura. The serous cavity around the testis was in fetal life continuous with the peritoneal cavity through the processus vaginalis (the tunica vaginalis and peritoneum being exactly equivalent), but as the muscles of the anterior abdominal wall are formed and become stronger, the processus becomes separated from the main peritoneal cavity. Attached to the lateral surface of the testis is the epididymis, into which the seminiferous tubules of the testis converge and eventually unite to form at its lower, and narrower end, the ductus (vas) deferens. The recess between the epididymis and the testis is the sinus of the epididymis. The covering of the testis, between it and the visceral layer of tunica vaginalis, is the tunica albuginea.
Unlike the scrotum, the testis is an organ of the posterior abdominal wall, like the kidney, and therefore:
• testicular arteries come directly from the aorta
• testicular veins drain to the IVC on the right and the renal vein on the left
• and, most importantly, lymphatic drainage is to nodes around the abdominal aorta, para-aortic nodes, and not to inguinal nodes like scrotal skin.
The testis develops high on the posterior wall of the embryonic coelom and subsequently descends through the inguinal canal so that at or soon after birth it should be in the scrotum. Its descent may be arrested at any stage. It may take a wrong turn after it has come through the inguinal canal: such ectopic testes are fairly easy to place in the scrotum since the spermatic cord is long enough. More difficult to deal with is the testis, which has not travelled far enough to have a sufficiently long spermatic cord for the testis to be placed in the scrotum. Testes which are allowed to remain ectopic are inclined to malignant change.
The testis may be retracted into the abdomen, out of harm’s way (presumably) – this is cremaster in action. The cremaster reflex may be elicited by gentle stimulation of the skin of the scrotum or anterior thigh, and plunging into cold water may cause retraction, although it is not usual for a man to retract his testes at will. It is of clinical significance in the young boy: a testis which has retracted in shock (as it were) because the hand palpating the scrotum is cold may be mistaken for an undescended testis.
If you suspect a testicular malignancy and find the inguinal nodes are enlarged, it is reasonable to assume that the malignancy has already spread from the testis to invade neighbouring scrotal skin, whence it has spread further to the inguinal nodes. Testicular malignancy is potentially lethal and it is as well for men to examine their testes as women do their breasts.
The testis may twist upon the spermatic cord resulting in occlusion of the blood supply. This is painful and is an emergency: the cord needs to be untwisted before the testis dies.
This is ligation and removal of a short length of the ductus (vas) deferens, usually for the purposes of birth control.
• Hydrocele. There may be a build-up of serous straw-coloured fluid between the layers of the tunica vaginalis (compare with pleural effusion). This is usually innocent: it simply needs to be drained by needle aspiration.
• Varicocele. Varicose veins of the pampiniform plexus and testicular veins may arise, more commonly (inexplicably, despite several theories) on the left than the right.
• Spermatocele. This is a fluid-filled cyst of the epididymis containing spermatozoa. It is uncommon.
A hernia is a condition in which internal structures are forced out through a weakness in the wall. In the inguinal region, abdominal contents (e.g. intestines, fat) may pass through the inguinal canal – a potential weak spot in the anterior abdominal wall. Since the canal is larger in the male than the female, inguinal hernias are commoner in the male.
• Indirect inguinal hernia. Abdominal contents pass through the deep inguinal ring and into the canal. They may be so large that they continue through the superficial ring, above and medial to the pubic tubercle, and present as a scrotal swelling. The neck (internal opening) of the hernia in this case would be through the deep inguinal ring, lateral to the inferior epigastric artery.
• Direct inguinal hernia. Abdominal contents bulge through the anterior abdominal wall between the deep inguinal ring and the midline, usually owing to a weak conjoint tendon. In this case, the neck of the hernia would be medial to the inferior epigastric artery.
It is not usually possible to distinguish these two hernias on clinical examination alone, except that a large scrotal hernia is more likely to be an indirect hernia.
• Congenital inguinal hernia. The potential space between the two layers of the tunica vaginalis may remain in continuity after birth with the peritoneal cavity. This is a congenital inguinal hernia: coils of intestine may surround the testis in the scrotum.
It may be difficult to distinguish between a scrotal swelling of testicular origin and a large inguinal hernia extending into the scrotum. If it is possible to ‘get above’ the swelling, it is not an inguinal hernia but something confined to the scrotum, for example a hydrocele.
Everything in the inguinal region of the female is much the same as in the male, except that it is all smaller and, as noted, inguinal hernias are less common in the female (but see Ch. 13; Femoral hernia, p. 210). The structure in the female which passes through the inguinal canal is the round ligament of the uterus, an insignificant structure derived from the gubernaculum (see an Embryology text for details). The labia majora of the female share the same blood supply (femoral, pudendal), nerve supply (genitofemoral, pudendal) and lymph drainage (mainly to inguinal nodes) as the scrotum in the male.
The intestines and associated organs were originally connected to the posterior abdominal wall by an elongated hilum, the dorsal mesentery. Subsequent changes in the disposition of abdominal viscera result in a complex arrangement of mesenteries and omenta. The transverse colon divides the abdominal cavity into supracolic and infracolic compartments. The areas on either side of the ascending and descending colons are the paracolic gutters. Other important areas of the peritoneal cavity are the lesser sac, the hepatorenal pouch and the subphrenic spaces.
Think of the gut tube and associated organs as pushing their way into the peritoneal cavity from behind, much as the lung pushes its way into the pleural cavity. The ‘hilum’ of the gut tube, where the parietal and visceral peritoneal layers meet, is elongated into a structure which connects the entire length of the gut tube to the dorsal body wall, and through it pass blood vessels, nerves, and lymphatics. This is the dorsal mesentery (Fig. 11.8).
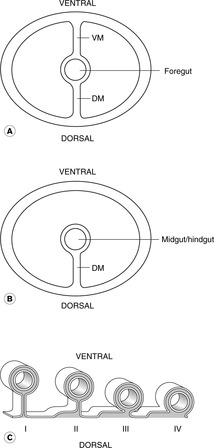
In the embryo, the gut tube enters the abdomen from the thorax passing behind a mass of mesoderm called the septum transversum, which subsequently becomes part of the diaphragm, liver and the connections between them and the ventral body wall. The upper part of the abdominal gut tube is attached not only to the dorsal body wall by the dorsal mesentery, but also to the ventral body wall by these derivatives of the septum transversum, which form the ventral mesentery (Fig. 11.8). This part of the gut tube is foregut and it extends distally as far as what will be the mid-portion of the duodenum. The remainder of the gut tube, midgut and hindgut, is connected to the dorsal body wall only by the dorsal mesentery, known simply as the mesentery: there is no ventral mesentery here.
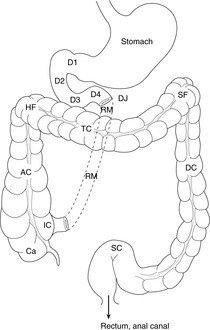
This simple layout of the gut tube in the peritoneal cavity is subsequently complicated by two factors. First, the tube elongates spectacularly and coils on itself within the abdomen; and secondly some parts of the gut tube then adhere to the dorsal body wall, thus losing their mesentery and becoming apparently retroperitoneal, an adjective meaning that the dorsal mesentery has been lost (Fig. 11.8). Clinically, this means that those parts of the alimentary canal that remain mesenteric are more mobile and may twist or herniate into other areas, while those that are retroperitoneal are more or less fixed. The final layout is shown in Figure 11.9.
Strictly speaking there is nothing in the peritoneal cavity except a thin layer of peritoneal fluid. Yet, you will hear: ‘the stomach is in the peritoneal cavity’ as you hear ‘the lungs are in the pleural cavities’ and ‘the heart is in the pericardial cavity’. The function of the peritoneal cavity is, like the pleural and pericardial cavities, to permit movement of the gut tube (postural, peristalsis, etc.) independent of movement of the body wall.
Abdominal cavity = peritoneal cavity. That part of the peritoneal or abdominal cavity that is within the pelvis is sometimes called the pelvic cavity, although it should more properly be the pelvic part of the peritoneal cavity.
Mesenteric = omental = epiploic = ligamentous (not to be confused with other uses of ligament). Which of these terms is used in any given situation is merely traditional.
• Supracolic compartment: superior to the transverse colon. This is usually taken to include the oesophagus, stomach, most of the duodenum, liver and biliary system.
• Infracolic compartment: inferior to the transverse colon. This includes the jejunum, ileum, caecum, ascending, descending and sigmoid colon, and rectum.
• Paracolic gutters: lateral to ascending and descending colons.
• Paravertebral gutters: between ascending and descending colons and the vertebral column.
• Hepatorenal (Morison’s) pouch: the superior end of the right paracolic gutter between liver and kidney.
• Subphrenic (subdiaphragmatic) and subhepatic spaces (Fig. 11.10). The liver and diaphragm developmentally are different parts of the same thing (septum transversum) and they remain attached to each other at the so-called bare area of the liver. The recesses of the peritoneal cavity partially separate the two structures. Naming of these is not consistent, but the system given here is as good as any:
– Posterior subphrenic space: posterior to the liver, between it and the posterior diaphragm. It is continuous with Morison’s pouch.
– Anterior subphrenic space: anteriorly between the liver and the diaphragm.
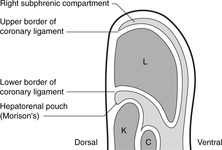
The anatomy of the liver, mainly a right-sided organ, means that these spaces are on the right side of the body.
• Lesser sac. Developmental changes mean that that part of the peritoneal cavity to the right of the (originally midline) stomach becomes at first behind the stomach (as the ventral surface of the stomach is displaced to the right), and then almost completely isolated from the rest of the peritoneal cavity as a result of the duodenum becoming adherent to the dorsal body wall. This is the lesser sac of the peritoneal cavity, behind the stomach, and the small communication between it and the rest of the peritoneal cavity is the epiploic foramen of Winslow (see later). The rest of the peritoneal cavity, with its supracolic and infracolic compartments, is the greater sac.
These pouches and sacs may be the sites of collection of inflammatory fluid which, particularly around the diaphragm, may go undiagnosed unless they are deliberately excluded – that is to say unless you think about the possibility of their involvement, you will miss them. This is particularly true of the areas between liver and diaphragm, and Morison’s pouch which, in a patient lying supine in bed, is the most dependent part of the peritoneal cavity. Fluid may collect here unless appropriate physiotherapy and regular postural changes are instituted.
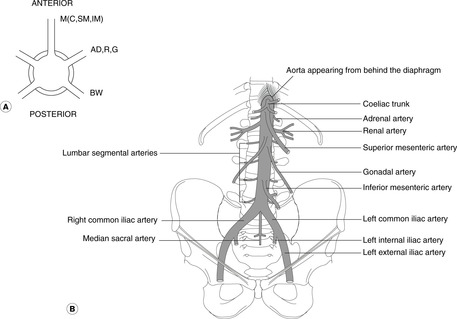
The aorta and inferior vena cava are on the posterior abdominal wall. Aortic branches serve the body wall (lumbar arteries), kidneys (renal arteries), gonads (ovarian and testicular arteries), and the gut tube (coeliac, superior mesenteric, inferior mesenteric arteries). The aorta divides into the common iliac arteries that supply pelvic organs and the lower limbs. The inferior vena cava is formed by the union of the common iliac veins and passes up on the right of the aorta to the liver where it is joined by hepatic veins, before penetrating the diaphragm and opening into the right atrium of the heart.
The aorta enters the upper abdomen slightly to the left of the midline behind the diaphragm at vertebral level T12. It passes down to about vertebral level L3/4 where it divides (surface marking: just below and to the left of the umbilicus in a recumbent patient) into the common iliac arteries. It is easily palpated in the upper abdomen between the umbilicus and the rib cage.
• Lumbar segmental arteries. There are paired, body wall branches, equivalent to the intercostals in the thorax. They are of no significance except that they give branches that pass into the vertebral canal to supply the spinal cord. Damage to the larger ones, for example in abdominal aortic surgery, may lead to spinal cord lesions.
• Renals, adrenals, gonadals. These are paired arteries, anomalous arrangements of which are common. The renals arise at about vertebral level L1 and you should study radiographs of them. The origin of the gonadals is more variable, but is usually about vertebral level L2/3.
• Mesenteric. These single, unpaired branches arise ventrally. There are three:
– Coeliac. Vertebral level T12. Supplies abdominal foregut (up to duodenal papilla) and structures which develop in foregut mesenteries: stomach, liver, spleen, most of the pancreas, duodenum as far as the papilla, greater omentum, lesser omentum.
– Superior mesenteric. Vertebral level T12/L1 (that is, immediately below the coeliac). Supplies midgut: distal duodenum, uncinate process of pancreas, jejunum, ileum, caecum, appendix, ascending colon, transverse colon, associated mesenteric structures.
– Inferior mesenteric. Vertebral level L3 (but more variable). Supplies hindgut: descending colon, sigmoid colon, rectum and upper part of anal canal.
• The common iliac arteries pass down and laterally towards the lower limbs. At the pelvic brim they divide to give external and internal iliac arteries.
The inferior vena cava is slightly to the right of the midline. It is formed from the two common iliac veins and passes upwards through the liver and diaphragm (at vertebral level T8) to enter the thorax. Its main tributaries are the renal, gonadal, adrenal and hepatic veins. Venous anatomy is in general much more variable than arterial anatomy, and anomalies are frequently encountered. A study of its complex embryology, though certainly not essential, will help to explain why. Suffice it here to say that the inferior vena cava may begin on the left and cross over the aorta to the right, or there may even be bilateral cavas up as far as the renal veins.
Segmental veins drain eventually to the azygos system and the superior vena cava; they have nothing to do with the inferior vena cava.
• The right sympathetic chain passes down from the thorax and comes to lie posterolateral to the inferior vena cava.
• The left sympathetic chain comes to be posterolateral to the aorta. Below the aortic bifurcation the chains continue over the pelvic brim in front of the sacrum and they unite to form the ganglion impar (unpaired). See section 11.13 (p. 151).
The oesophagus enters the abdomen behind the diaphragm at vertebral level T10 slightly to the left of the midline surrounded by fibres from the right diaphragmatic crus forming a sphincter mechanism: the cardio-oesophageal sphincter. See section 11.9 (p. 132).
This arises when part of the stomach pushes its way up into the thorax through the oesophageal opening in the diaphragm. The two types, rolling and sliding, are dealt with in clinical texts. Hiatus hernias may give rise to epigastric discomfort. This is not the same as a congenital diaphragmatic hernia, in which there is a defect in one or both sides of the diaphragm.
The size and position of the stomach vary depending upon body shape, degree of distension, and posture. The five areas of the stomach (do not worry about the precise boundaries) are:
• cardia (around the oesophageal opening)
• fundus (above the level of the oesophageal opening)
• body (central portion)
• antrum (lower part)
• pylorus (the most distal part), the thickened sphincter mechanism controlling passage of stomach contents to the duodenum. The pylorus normally lies at about vertebral level L1, the transpyloric plane.
The left border is the greater curvature and the right the lesser curvature.
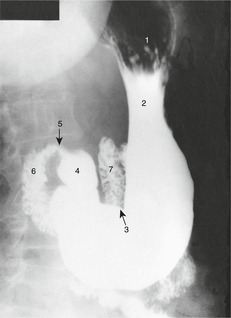
The alimentary canal can be demonstrated radiographically with the use of radio-opaque barium compounds. A barium swallow demonstrates the mouth, pharynx and oesophagus. In a barium meal the stomach and small intestines are displayed after an appropriate time interval.
As explained earlier, the original ventral border of the stomach is attached to the ventral body wall by the ventral mesogastrium. This border becomes the lesser curvature, and the ventral mesogastrium (mesogastrium = mesentery of the stomach) becomes, from stomach ventrally, lesser omentum, liver and falciform (sickle-shaped) ligament. The lesser omentum moves during development so that by the time of birth it lies in a more-or-less coronal plane, and behind it and the stomach is the lesser sac of the peritoneal cavity, which opens into Morison’s pouch of the greater sac through the epiploic foramen of Winslow.
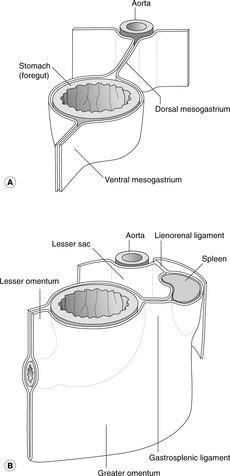
Between spleen and stomach the mesentery is known by two names. Above, it is the gastrosplenic ligament. Below, it grows down to form a double layer of omental (mesenteric) tissue partly covering the intestines – the greater omentum. This is, amongst other things, a fat store and may become very large – regrettably so in some middle-aged people (including the author). The greater omentum is, with the stomach and lesser omentum, part of the anterior wall of the lesser sac, and, again in development, it becomes adherent to the mesentery of the transverse colon – the transverse mesocolon – so that the transverse colon is attached to the under surface of the greater omentum.
This is like three and a half sides of an approximate rectangle, inside which is the head of the pancreas. There are four parts.
• First part. This passes backwards and horizontally, becoming retroperitoneal (i.e. loses its mesentery). It passes anterior to the common bile duct and the gastroduodenal artery. Posterior duodenal ulcers may erode this, causing haemorrhage.
• Third part. This is retroperitoneal and passes horizontally to the left at about vertebral level L2/3, crossing the midline in front of the abdominal aorta below the origin of the superior mesenteric artery. Disease of either duodenum or aorta can result in an aortoduodenal fistula presenting as bleeding into the intestine.
• Fourth part. This, also retroperitoneal, turns upwards on the left side of the midline and at about vertebral level L1 turns to the left and once again becomes mesenteric as the jejunum: this is the duodenojejunal flexure (‘d–j flexure’) or junction. It is anchored (some say) by a few smooth muscle fibres in the so-called ligament of Treitz, which passes down from the diaphragm to the duodenojejunal junction.
The exocrine acini secrete into a duct system that begins in the tail and proceeds to the right. As it enters the head it turns inferiorly to join the common bile duct and enters the duodenum at the papilla. There may be an accessory pancreatic duct opening above the main duct.
This is from branches of the coeliac and superior mesenteric arteries (see later).
• Pancreatic pain is often felt in the back as well as generally in the abdomen anteriorly.
• Inflammation of the pancreas (pancreatitis) may result in a collection of inflammatory fluid in the lesser sac – a pancreatic pseudocyst.
• Cancer of the head of the pancreas may result in blockage of the common bile duct as it approaches the duodenal papilla.
• The pancreas develops from two outgrowths of foregut which, after some rotation around the gut tube, fuse. Congenital anomalies include a condition in which pancreatic tissue forms a ring around the duodenum – annular pancreas. This may cause duodenal obstruction.
This is situated at the back (not the side) on the left, related to ribs 9, 10 and 11. It extends between vertebral levels T12–L2 under the left dome of the diaphragm. It is anterior to the left costodiaphragmatic recess of the pleural cavity. It does not normally extend any further anteriorly than the midaxillary line and is therefore not normally palpable. It is about the size of a clenched fist and, having developed in the dorsal mesogastrium, is attached to the dorsal body wall by the splenorenal ligament and to the stomach by the gastrosplenic ligament. At its hilum (vertebral level L1, transpyloric plane) it is in contact with the tail of the pancreas, which extends into the splenorenal ligament, through which the splenic vessels pass between the posterior abdominal wall and the spleen.
The spleen is in danger from trauma to the left lower rib cage, particularly ribs 9, 10 and 11. A ruptured spleen may cause fatal haemorrhage since, as part of the haematological policing system of the body, it has a profuse blood supply. It may become enlarged in haematological conditions or liver disease. As it enlarges it becomes palpable at the left subcostal margin, but you should note that by the time it does so it is already about three times larger than normal. It may enlarge further diagonally down towards the right iliac fossa. Such a huge spleen may be found in haematological diseases (e.g. sickle cell anaemia, leukaemia), and, lacking a palpable border in the place where it might be expected because it is so large, it may escape detection.
The liver occupies the right and central upper abdomen, roughly from the fourth intercostal space (nipple in a lean male) to the costal margin. A very rough approximation is to draw a triangle whose angles are the two nipples and the tenth costochondral junction. Posteriorly, it is somewhat smaller: to map its surface projection, join the two inferior angles of the scapulas to the midpoint of the right eleventh rib.
The liver and most of the diaphragm develop from the septum transversum, and part of the liver remains in direct contact with the diaphragm with no intervening peritoneum: this is the bare area. The margins of the bare area, where the hepatic visceral peritoneum is reflected on to the under surface of the diaphragm, are known as the coronary ligament, and the right and left extremities of this are the right and left triangular ligaments.
Posteriorly, the liver is supported mainly by the inferior vena cava and the hepatic veins. Anteriorly (Fig. 11.18) it is connected to the anterior abdominal wall by the falciform ligament which has a free lower border extending from the internal aspect of the umbilicus to the inferior surface of the liver. This border contains the ligamentum teres – the obliterated umbilical vein that in fetal life conveyed oxygenated blood from the placenta to the fetus.
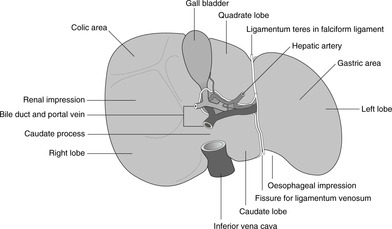
There are four anatomical lobes: right, left, quadrate and caudate. Their boundaries are not demarcated on the anterosuperior surface of the liver, but are clearer on the inferior, or visceral, surface (Fig. 11.19). This surface displays an H-shaped group of fissures. The crossbar of the H is the porta hepatis, the area anterior to it the quadrate lobe and posterior to it the caudate lobe.
• The left-sided limb of the H is a deep fissure receiving:
– the falciform ligament (with the ligamentum teres in its free edge), and
– part of the lesser omentum from the stomach, attached deep in this fissure to the obliterated ligamentum venosum (a continuation in the fetus of the umbilical vein).
• The right limb of the H is made up of two fossas, anteriorly for the gall bladder and posteriorly for the inferior vena cava.
• The quadrate lobe lies between the falciform ligament and the fossa for the gall bladder.
Physiologically and functionally, these anatomical lobes are of no significance. Functionally, the liver is divided into lobes and segments similar to the bronchopulmonary segments of the lung, each with its own branches of the hepatic artery and portal vein, and each with its own tributaries of the hepatic vein and the biliary tree. Knowledge of these is useful for surgeons but is not required for undergraduates.
The inferior vena cava passes through the bare area of the liver and the diaphragm (vertebral level T8) to enter the thorax and the right atrium of the heart. In this region the right adrenal gland is posterior to the IVC and intimately related to the bare area of the liver.
The biliary tree conveys the exocrine products of the liver (bile) to the duodenum. The gall bladder is a blind diverticulum of the biliary tree for the purposes of bile storage. The right and left hepatic ducts unite to form the common hepatic duct. The cystic duct from the gall bladder joins this to form the common bile duct. There is some variation in the layout of this duct system: the important thing is that the common bile duct passes down in the free edge of the lesser omentum, then posterior to the duodenum and into the substance of the head of the pancreas. It turns to the right and unites with the pancreatic duct. There is then a small widening, the ampulla of Vater, before the sphincter mechanism (sphincter of Oddi), which protrudes slightly into the left side of the second part of the duodenum as the duodenal papilla.
This arises when the normal passage of bile into the duodenum is blocked, either partially or wholly. It may arise within the liver (intrahepatic) or outside it (extrahepatic). Extrahepatic causes include gallstones, which find their way into the common bile duct and then block it, or cancer of the head of the pancreas, compressing the common bile duct from the outside as it passes through the head of the pancreas. In these cases with severe or complete blockage of the biliary tree, bile pigments will not reach the duodenum so the faeces will be lighter coloured than normal; biliary enzymes will not reach the intestines so that fat will be poorly digested and the faeces will be fatty (steatorrhoea) and float in the toilet bowl; bile pigments, instead of being in the intestines, will be absorbed into the bloodstream, so the patient appears yellow, and bile pigments are excreted in the urine, so the urine is dark. The combination of pale stools and dark urine means obstructive jaundice. Associated with episodes of excruciating pain, it probably means gallstones in the duct; associated with lassitude and weight loss it probably means cancer of the head of the pancreas.
The coeliac artery arises from the aorta at vertebral level T12, and supplies all the abdominal foregut and derivatives. There are three branches: splenic, hepatic, left gastric.
• Splenic: passes in the posterior wall of the lesser sac through or along the top of the pancreas (giving branches to it) and through the lienorenal ligament to the spleen. Near the spleen it gives short gastric arteries that pass in the gastrosplenic ligament to the fundus of the stomach, and the left gastroepiploic, which supplies the greater omentum and the greater curvature of the stomach.
• Common hepatic (usually simply hepatic): passes to the liver in the free edge of the lesser omentum. It gives:
– right gastric: lesser curvature
– gastroduodenal: passes inferiorly, behind the first part of the duodenum, and divides into the right gastroepiploic (for the greater curvature) and the superior pancreaticoduodenal which runs between the head of the pancreas and the duodenum, supplying them both
– cystic: to the gall bladder
– right and left hepatic arteries (terminal branches).
• Left gastric: lesser curvature and terminal oesophagus.
Note that the duodenum distal to the duodenal papilla is a midgut derivative. It is therefore supplied by branches of the superior mesenteric artery, in particular the inferior pancreaticoduodenal, which runs in the groove between pancreas and duodenum, anastomosing with the superior pancreaticoduodenal.
• Anterior – structures in the free edge of the lesser omentum: portal vein (behind), common hepatic artery (front left), common bile duct (front right).
• Superior – caudate lobe of liver.
• Posterior – inferior vena cava.
• Inferior – duodenum (first part).
All blood passing to the liver enters through either the hepatic artery (freshly oxygenated, from the aorta) or the portal vein (from the intestinal bed). Both these vessels pass in the free edge of the lesser omentum. Bleeding from the liver, therefore, can be stemmed by compressing the free edge of the lesser omentum (Pringle’s manoeuvre). Should bleeding continue, it is likely that the inferior vena cava has been damaged.
Lymph from foregut structures drains to coeliac nodes, although in reaching them other structures may be involved. The lymph drainage of the stomach is particularly important because of stomach cancer and, as elsewhere, it mirrors the arterial supply:
• lymph from the greater omentum passes to splenic and pancreatic nodes before reaching coeliac nodes
• as well as draining to the coeliac nodes, lymph from the lesser curvature may pass retrogradely to the liver, leading to hepatic involvement – this is not uncommon.
From the coeliac nodes, lymph passes to the cisterna chyli, the thoracic duct and its termination in the formation of the left brachiocephalic vein. In some cases of upper abdominal malignant disease, particularly stomach cancer, involvement of left supraclavicular nodes may occur, presumably because of their proximity to the termination of the main thoracic duct. This, when present, is known as Virchow’s node.
Midgut and hindgut extend from the second part of the duodenum to the anal canal. They receive blood from the superior and inferior mesenteric arteries, and venous blood drains to the portal system. Lymph drains to mesenteric nodes, thence to preaortic nodes and the cisterna chyli.
You should:
• describe the disposition of the jejunum and ileum
• describe the disposition and surface anatomy of the caecum, ascending colon, transverse colon, descending colon and sigmoid colon
• describe the blood supply of midgut and hindgut and the importance of the marginal artery.
The midgut extends from the duodenal papilla to (roughly) the distal end of the transverse colon (splenic flexure), and hindgut extends from there to the pectinate (dentate) line of the anal canal. For the third and fourth parts of the duodenum, see above.
At the duodenojejunal flexure, the gut tube once again becomes mesenteric and the first (about) two-fifths of the mesenteric small bowel is the jejunum, the remainder the ileum. Anatomically they may be differentiated by the pattern of arteries in the mesentery, and the jejunal walls are somewhat thicker, but neither of these matters to anyone except surgeons. The mesentery of the jejunum and ileum is known simply as ‘the mesentery’. Originally in the midline, it has shifted during development so that it runs from above left to bottom right. Branches of the superior mesenteric vessels pass in it.
Inside the jejunum, the mucosa forms prominent folds: the plicae circulares.


