The big picture203
13.2 Hip joint, gluteal region and upper thigh205
13.3 Knee joint, movements, muscles, posterior thigh, popliteal fossa213
13.4 Ankle joint and movements: posterior, anterior and lateral compartments of leg217
13.5 Foot222
13.6 Venous drainage of the lower limb225
13.7 Innervation, nerve testing, surface anatomy226
13.1. The big picture
First, some words of caution.
Parts of this chapter assume that you have already studied the upper limb. When comparing the lower limb with the upper, there are some potentially confusing issues that you need to keep in mind:
• Thigh, leg. ‘Thigh’ means lower limb from groin to knee. ‘Leg’ means knee to ankle, not the entire lower limb.
• Lateral, medial, tibial, fibular. In the lower limb, unlike the upper limb, lateral and medial are unambiguous. Nevertheless, in the leg, the terms tibial (medial) and fibular or peroneal (lateral) are also used.
• Anterior, posterior, flexors, extensors. During development, the lower limb rotates medially so that muscles and skin supplied by anterior divisions of ventral rami become medial (above the knee) or posterior (below the knee), and muscles and skin supplied by posterior divisions come round to be lateral and in front. So, extensors are at the front, flexors at the back, the knee points forwards (not backwards like the elbow) and the dorsum of the foot is at the front, not the back.
• Peroneal (from Greek) and fibular (from Latin) are synonymous. Peroneus and peroneal are used by many older books but are increasingly being replaced by fibularis and fibular. If you use peroneal, spell it correctly: perineal means something else altogether.
Arteries (see Fig. 7.1, p. 44; Fig. 13.1)
Arterial blood to the lower limb comes from the femoral artery and its branches, with the gluteal arteries (from the internal iliac) supplying the gluteal region.
• Femoral. This is the principal artery to the lower limb. It enters the thigh behind the midpoint of the inguinal ligament and descends into the popliteal fossa where it becomes the popliteal.
• Profunda femoris. The profunda femoris is an early branch of the femoral. It supplies the thigh and gives a series of branches which encircle the femur and contribute to the supply of the hip joint.
• Popliteal. At the lower border of the popliteal fossa the popliteal artery divides into anterior and posterior tibial arteries.
• Anterior tibial. This descends in the anterior (extensor) compartment becoming the:
• Dorsalis pedis artery of the foot.
• Posterior tibial. This descends in the posterior (flexor) compartment, entering the foot posteromedial to the ankle and dividing into:
• Medial and lateral plantar arteries. The lateral plantar anastomoses with the continuation of the dorsalis pedis that passes into the sole between the first (big toe) and second metatarsals.
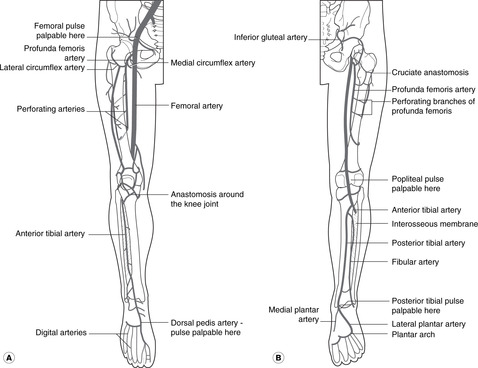
Palpable pulses. These are the femoral, popliteal, dorsalis pedis, and posterior tibial.
Veins, deep fascia, fascia lata (see Fig. 7.2, p. 45)
Venous blood drains to the femoral vein, thence to the external iliac and inferior vena cava. As in the upper limb there are deep and superficial systems.
• Superficial veins are immediately subcutaneous, superficial to the deep fascia. Although the pattern of superficial veins is variable, one is particularly important: the great (or long) saphenous vein (saphenous: from Greek, meaning visible), which empties into the femoral vein by passing through a defect in the deep fascia at the top of the thigh, the saphenous opening. Note that the deep fascia of the thigh is called the fascia lata.
• Deep veins accompanying the arteries (venae comitantes) converge to form the popliteal vein, which in turn becomes the femoral. They receive blood from superficial veins through connections which, since they penetrate the deep fascia, are known as perforating veins, or simply perforators.
Since we stand on our feet, venous return from the lower limb is often against gravity. Venous disease of the lower limb is common and the mechanism of venous return is important. It is dealt with in section 13.6 (p. 225).
Lymph (see Fig. 7.4, p. 46; Fig. 13.2)
All lymph drains to inguinal nodes.
• From the medial side, lymph drains directly to inguinal nodes.
• From the lateral side, lymph drains to the popliteal nodes behind the knee, thence to inguinal nodes.
• From inguinal nodes, lymph passes to external iliac nodes, thence to para-aortic nodes, the cisterna chyli and thoracic duct to the venous system at the origin of the left brachiocephalic vein.
Nerves
• From the lumbar plexus (L1–5): to the anterior and medial thigh – hip flexion and adduction and knee extension. Revise the lumbar plexus (Fig. 11.26, p. 134).
• Dermatomes and myotomes. As in the upper limb, the muscles and skin supplied by one segmental nerve are not adjacent as in the trunk. The dermatomes (sensory) are shown in Figure 6.6 (p. 36).
13.2. Hip joint, gluteal region and upper thigh
The head of the femur articulates with the acetabulum of the hip bone. The hip joint is surrounded by large muscles, bones, joint and ligaments reflecting the forces imposed as a result of our bipedal gait. The blood supply of the joint and the head of the femur is an important consideration in patients with fractured femoral necks. Hip flexion and medial rotation are performed by muscles in and around the femoral region; extension and lateral rotation by posterior muscles (gluteal and hamstrings). The principal nerves in this region are the femoral anteriorly, vulnerable to injury in the femoral triangle, and the sciatic posteriorly, at risk in ill-judged injections and posterior dislocations of the hip.
You should:
• describe the structure of the hip joint and how it may be injured
• describe the blood supply of the joint and head of the femur
• list the principal muscle groups acting on the joint, and their innervation
• describe the structures in the femoral triangle, and the anatomy of femoral hernia
• describe the surface markings of the sciatic and femoral nerves, and the femoral artery in the femoral triangle
• explain the effects of damage to the femoral and sciatic nerves.
Bones
Sacrum (see Fig. 11.29, p. 137)
• Posterior surface: provides attachment for gluteus maximus, and foramina for dorsal rami of sacral nerves are evident (not important).
• Anterior surface: provides attachment for piriformis, and foramina for ventral rami of sacral nerves are evident.
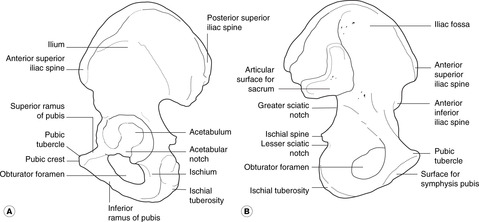
Hip bone (see Fig. 11.29, p. 137; Fig. 13.3)
• Anterior surface of ilium: provides attachment for iliacus which, with psoas from the vertebral column, forms the main hip flexor, iliopsoas.
• Posterior (gluteal) surface of ilium: provides attachment for gluteus medius and gluteus minimus.
• Ischial tuberosity: provides attachment for posterior muscles of the thigh (hamstrings); these extend the hip and flex the knee.
• Pubic symphysis: a midline secondary cartilaginous joint.
• Pubic crest and pecten: provide attachment for pectineus (not important).
• Obturator foramen: this is a large defect closed by membrane in which is a small hole allowing the obturator neurovascular bundle to pass between pelvis and medial thigh.
• Ischiopubic ramus (lower border of obturator foramen formed by ramus of ischium and inferior ramus of pubis): provides attachment for adductor muscles.
• Acetabulum: articular surface for the head of the femur. The acetabular notch allows a branch of the obturator artery to enter the round ligament (ligamentum teres) of the head of the femur, which attaches the femur to the hip bone. The components of the hip bone, the ilium, ischium and pubis, meet in the centre of the acetabulum, the three parts fusing at about 16 years of age.
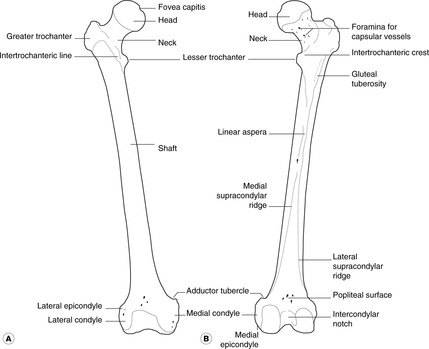
Femur (Fig. 13.4)
• Head: this articulates with the acetabulum. A small pit, the fovea capitis, marks the attachment of the round ligament.
• Neck: note the many small foramina which allow blood vessels to enter the bone.
• Lesser trochanter: for the distal attachment of iliopsoas.
• Greater trochanter: provides attachment for gluteus medius and gluteus minimus.
• Trochanteric line, the ridge on the anterior surface of the femur connecting the two trochanters: the iliofemoral ligament of the hip joint capsule is attached here.
• Trochanteric fossa, between the greater trochanter and the femoral neck: provides attachment for piriformis, obturator externus and obturator internus.
• Gluteal tuberosity, on the posterior aspect of femur: provides attachment for part of gluteus maximus.
• Linea aspera: provides attachment for adductors, vastus muscles and the short head of biceps femoris.
• Adductor tubercle: provides attachment for adductor and vastus muscles.
• Shaft: this is smooth, except for the linea aspera posteriorly.
Hip joint (Fig. 13.5, Fig. 13.6 and Fig. 13.7)
This is a ball and socket synovial joint. The acetabulum is deepened by the acetabular labrum, a rim of hyaline cartilage which, with the transverse acetabular ligament, closes the acetabular notch.
 |
| Fig. 13.6 |
 |
| Fig. 13.7 |
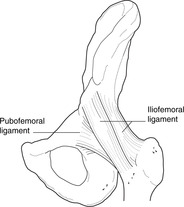
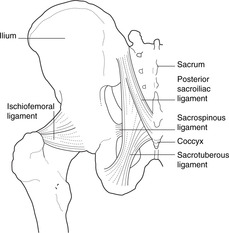
Joint capsule: iliofemoral, pubofemoral and ischiofemoral ligaments (Figs 13.6, 13.7)
The fibrous capsule is attached proximally to the acetabular margin and distally to the intertrochanteric line on the anterior surface of the femur and about halfway up the femoral neck above and behind. Inferiorly, it extends some way down the medial border of the femur to provide sufficient slack capsule which can be taken up on abduction. The fibres of the capsule form three strong ligaments:
• Iliofemoral ligament. Attachments: anterior inferior iliac spine and acetabular margin (proximally)–intertrochanteric line (distally). This strengthens the front of the joint capsule.
Blood supply of head of femur and hip joint: cruciate and trochanteric anastomoses
• Capsular (retinacular) vessels arise from the cruciate and trochanteric anastomoses posterior to the hip joint and neck of the femur. These receive blood from the gluteal and obturator arteries (from the internal iliac), and from circumflex femoral branches of the profunda femoris artery.
• Terminal branches of the nutrient artery from the shaft. In children these do not reach the femoral head, since vessels never cross the epiphyseal plate of developing bone.
• Artery of the round ligament (from the obturator). This is never sufficient to keep the femoral head viable if the other sources of blood are compromised (e.g. in fractures of the femoral neck).
Avascular necrosis of the femoral head may occur after a fracture of the femoral neck. It may also occur in children for reasons that are not entirely clear: this is Perthes’ disease.
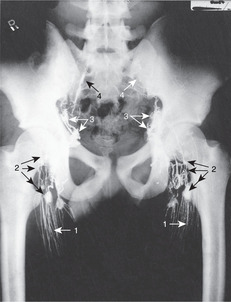
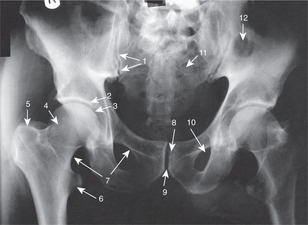
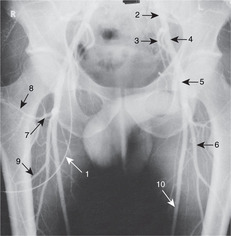
Shenton’s line
On a radiograph, the lower margin of the femoral neck appears to be continuous with the iliopubic ramus (upper margin of the obturator foramen) of the hip. This is Shenton’s line (Fig. 13.5). If it appears to be discontinuous, it is likely that the femoral neck is fractured.
Nerve supply: hip pain and the knee
Branches of femoral, obturator, sciatic and gluteal nerves. Some of these nerves also give branches to the knee joint and pain from the hip may be referred to the knee. So, if you have a patient with pain in the knee, you must exclude disease of the hip.
Flexion and adduction at the hip, femoral triangle, adductor compartment
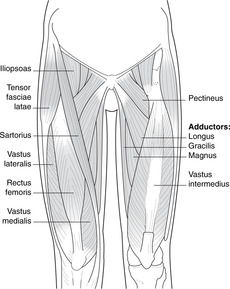
Flexion (Fig. 13.8)
Nerve supply: femoral nerve (L2–4) and direct branches from the lumbar plexus.
• Iliopsoas. Attachments: anterior surface of iliac crest (iliacus) and lumbar vertebral column and discs (psoas)–lesser trochanter. It is the principal flexor supplied directly from the lumbar plexus. It passes deep to the inguinal ligament.
• Sartorius. Attachments: anterior superior iliac spine–medial side of upper end of tibia.
• Pectineus. Attachments: superior border (pecten) of pubis–lesser trochanter with iliopsoas. It also has an adductor role and receives fibres from the obturator nerve as well as the femoral.
 |
| Fig. 13.8 |
Adduction (Fig. 13.8)
Nerve supply: obturator nerve, L2, 3, 4.
• Adductor longus. Attachments: below pubic tubercle–linea aspera of femur.
• Gracilis (strictly speaking, adductor gracilis). Attachments: inferior ramus of pubis–medial side of tibia.
• Adductor brevis. Attachments: inferior ramus of pubis–linea aspera of femur.
• Adductor magnus. Attachments: ischiopubic ramus–linea aspera and adductor tubercle of femur. Just above the attachment to the adductor tubercle the muscle fibres part to allow the femoral artery and vein to pass between the anterior and posterior compartments: the femoral/popliteal boundary.
Femoral region (Fig. 13.9)
• At the midpoint of the inguinal ligament, the femoral artery passes from abdomen to thigh. Lateral to it is the femoral nerve and medial the femoral vein. Medial to the vein is:
• The femoral canal – a short extension of the abdominal cavity beneath the inguinal ligament into the thigh. It contains nothing in particular other than a few lymph nodes. Medial to it is:
• The lacunar ligament, an extension of the inguinal ligament which passes on to the superior pubic ramus.
• The femoral ring is the opening of the femoral canal to the abdominal cavity.
• The femoral sheath encloses the canal, the vein and the artery, but not the nerve.
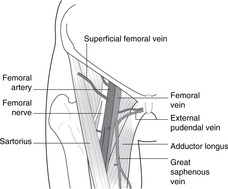
Femoral triangle and vessels (Figs 13.9, 13.10)
• The base of the triangle is the inguinal ligament, the medial border of sartorius laterally, and the medial border of adductor longus medially. Its floor is formed by (from above down) iliopsoas, pectineus and adductor longus.
• The femoral artery passes to the apex of the femoral triangle and then runs for a short distance under sartorius to the gap in adductor magnus where it enters the popliteal fossa. The subsartorial ‘canal’ is also called the adductor or Hunter’s canal.
• The profunda femoris artery arises in the upper part of the femoral triangle and is large, its size reflecting the importance of the thigh muscles and hip joint. It provides a series of arteries that encircle the femur, the uppermost of which, the circumflex femorals, contribute to the cruciate and trochanteric anastomoses supplying the hip joint. The lower branches perforate the fascia between the anterior and posterior thigh muscles and are known as perforating arteries (not to be confused with perforating veins joining the deep and superficial venous systems).
Femoral and obturator nerves (Figs 13.11, 13.12)
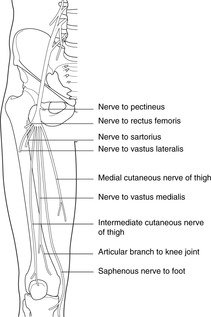
• The femoral nerve enters the thigh immediately lateral to the femoral pulse at the inguinal ligament. It divides into numerous branches:
– to knee extensors
– medial and intermediate cutaneous nerves of the thigh (the lateral cutaneous is a separate nerve, see Fig. 11.26, p. 134)
– saphenous nerve (sensory), which continues through the subsartorial canal and then becomes superficial, running down the medial side of the lower thigh and leg with the great saphenous vein to the foot. It supplies a strip of medial skin over and around it and thus a branch of the femoral nerve carries L4 fibres all the way to the foot.
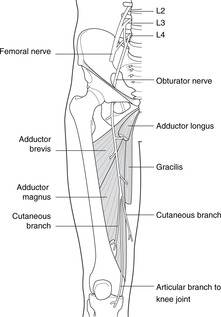
• The obturator nerve enters the thigh through the obturator foramen and supplies:
– hip adductor muscles
– skin of the upper medial thigh
– sensory fibres to the knee joint.
• Both femoral and obturator nerves are formed from ventral rami of L2, 3, 4, the obturator from anterior divisions, and the femoral from posterior divisions. Posterior divisions at the front? Yes: remember the embryonic medial rotation: see the beginning of this chapter.
Femoral hernia
Abdominal contents (e.g. fat, gut) may find their way into this and form a femoral hernia. It would be deep to the deep fascia of the thigh – the fascia lata – and may not be evident upon physical examination until it is large enough to protrude through the saphenous opening in the fascia lata which transmits the termination of the great saphenous vein. The hernia would present as a swelling in the thigh below and lateral to the pubic tubercle (an inguinal hernia would be above the pubic tubercle). Surgical procedures to reduce a femoral hernia may involve cutting the lacunar ligament to allow more room for manoeuvre: beware an accessory obturator artery passing from the external iliac artery to the obturator foramen.
Stab wounds in the femoral triangle
The femoral vessels and nerve are at risk and the potential for serious injury is great: paralysis of knee extension with resultant difficulties in locomotion, and potentially fatal haemorrhage. Apart from criminal attacks, those who wield long knives professionally (e.g. butchers) may injure themselves here: chain mail protection is available.
 |
| Fig. 13.11 |
 |
| Fig. 13.12 |
Hip abduction, rotation, extension; gluteal region
Abduction and medial rotation (Fig. 13.13)
These muscles are hip abductors: if you contract them whilst seated, this is what they do. But if you are standing with, say, your right foot on the ground and you contract them on the right, they will raise the opposite side of the pelvis, allowing you to lift your left foot. This is their principal function: the hip abductors contract on the weightbearing side during locomotion to allow body weight to be supported on the ipsilateral lower limb. If they are weakened or paralysed (e.g. poliomyelitis affecting L4, 5, S1), the pelvis will dip to the non-weightbearing side resulting in a waddling gait, the Trendelenburg gait (not to be confused with the waddling gait that workers in the fashion industry, and others, try hard to acquire).
• Tensor fasciae latae. Attachments: lateral iliac crest–lateral longitudinal thickening of fascia lata, the iliotibial tract, which passes between the ilium and the lateral condyle of the tibia. Many authorities regard this muscle as an extensor, but my eyes and hands tell me it is an abductor, and it is supplied by the superior gluteal nerve.
Extension (Fig. 13.13)
• Gluteus maximus. Attachments: posterior surface of iliac crest, sacrum, coccyx, sacrotuberous ligament–femur and tibia via iliotibial tract (see below).
Nerve supply: inferior gluteal nerve, L5 S1, 2.
Gluteus maximus is the big superficial muscle of the backside. Less than one-quarter of its fibres are attached to the femur, to the gluteal tuberosity just below the greater trochanter. Most fibres pass to the iliotibial tract of the fascia lata (see above). Gluteus maximus is a powerful extensor of the hip, used particularly for antigravity movements such as rising from the kneeling or sitting position, or climbing stairs.
• Hamstrings (semitendinosus, semimembranosus, biceps femoris). Attachments: ischial tuberosity–femur, tibia and fibula.
Nerve supply: tibial and common fibular nerves, L5, S1, 2, 3.
These hip extensors are also important knee flexors and are considered in detail in that section.
Lateral rotation: direct branches of L4–S2 (Fig. 13.13)
None of these muscles is particularly important.
• Piriformis. Attachments: anterior aspect of sacrum–greater trochanter (through greater sciatic foramen).
• Obturator externus. Attachments: outer margins of obturator foramen and membrane–trochanteric fossa.
• Obturator internus. Attachments: inner margins of obturator foramen and membrane–trochanteric fossa. This muscle turns a right angle through the lesser sciatic foramen. As it emerges it is joined above and below by fibres attached to the margins of the foramen, the superior gemellus and inferior gemellus (definitely not important).
• Quadratus femoris: ischial tuberosity–greater trochanter.
Other features of gluteal region and the hip
Greater and lesser sciatic foramina
The greater sciatic foramen transmits:
• the superior gluteal nerve and vessels above piriformis
• the inferior gluteal nerve and vessels, the pudendal nerve and vessels, and (usually) the sciatic nerve below piriformis. The pudendal nerve immediately then dives into the lesser sciatic foramen to pass in the ischioanal fossa of the perineum.
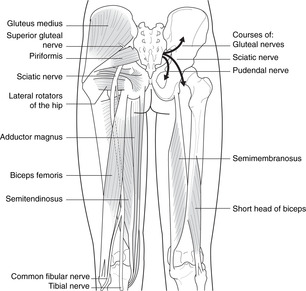
Sciatic nerve (Fig. 13.13)
• The nerve roots of L4–S3 form two large nerves, the tibial (anterior divisions supplying flexors) and the common fibular or fibular (posterior divisions supplying extensors). These nerves, although separate entities, are usually bound together as the sciatic nerve, the two components separating in the popliteal fossa.
However, they may be separate throughout their length, with the common fibular nerve passing above or through piriformis and the tibial through or below piriformis.
• The sciatic nerve in the gluteal region is immediately posterior to the hip joint capsule and may be damaged by posterior hip dislocations.
Sciatic nerve surface markings: injections
Surface markings of sciatic nerve:
• halfway between posterior superior iliac spine and ischial tuberosity, to
• halfway between ischial tuberosity and greater trochanter.
To be sure to avoid the nerve, intramuscular injections must be given in the upper outer quadrant of the backside.
13.3. Knee joint, movements, muscles, posterior thigh, popliteal fossa
Bones
Distal femur (Fig. 13.14)
• Articular condyles: articulate with the tibia, the medial is bigger than the lateral. The patella articulates anteriorly.
• Linea aspera: this provides attachment for vastus muscles and the short head of biceps femoris. The linea aspera widens to form the:
• Popliteal surface, immediately related to the popliteal artery.
• Intercondylar notch: provides attachment for cruciate ligaments.
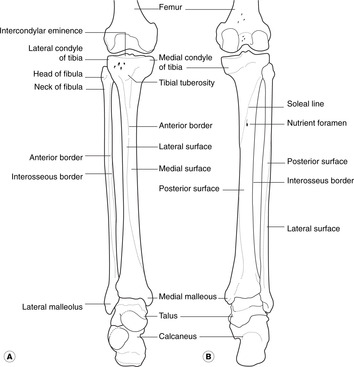
Proximal tibia (Fig. 13.14)
• Articular surfaces: receive the femoral condyles, the medial is bigger than the lateral.
• Intercondylar eminence: provides attachments for cruciate ligaments and menisci.
• Tibial tuberosity: provides attachment for the patellar ligament.
• Facet for articulation of fibula (superior tibiofibular joint).
Proximal fibula (Fig. 13.14)
• Head: this articulates with the tibia.
• Neck: this is related to the common fibular nerve.
Patella
This is a sesamoid bone in the tendon of quadriceps femoris.
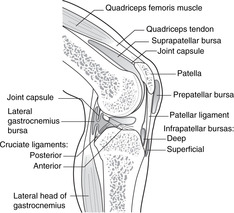
Knee joint
Synovial cavity
The synovial cavity has medial and lateral compartments that communicate anteriorly behind an infrapatellar fat pad. It extends superiorly for about a handsbreadth above the upper margin of the patella – the suprapatellar bursa (see below). There are two articulations between the tibia and femur, right and left, and one between the anterior femur and the patella.
Menisci (semilunar cartilages) and collateral ligaments (Figs 13.15, 13.16)
• Medial and lateral menisci form partial cushions between tibia and femur and are attached to the intercondylar eminence of the tibia.
• The medial collateral ligament, a broad and flat band, is a thickening of the knee joint capsule and is attached to the medial meniscus. It is taut in knee extension and prevents knee abduction.
• The lateral collateral ligament is a cord-like structure, attached neither to the lateral meniscus nor the knee joint capsule. It is taut in knee extension and prevents knee adduction.
• The medial meniscus is more commonly injured in twisting (‘cartilage’) injuries than the lateral, partly because it is less mobile than the lateral and can not move out of the way.
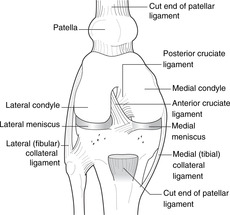
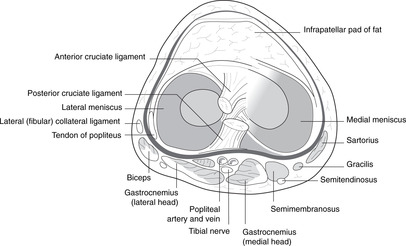
Cruciate ligaments (Figs 13.16, 13.17)
• The anterior cruciate ligament is attached to the anterior intercondylar area of the tibia and passes upwards, backwards and laterally to the lateral side of the intercondylar notch of the femur. It limits anterior movement of the tibia on the femur (or posterior movement of the femur on the tibia). We can manage without it if it is torn.
• The posterior cruciate ligament is attached to the posterior intercondylar area of the tibia and the lateral meniscus. It passes upwards, forwards and medially (the two ligaments thus making a cross – hence the name) to the medial side of the intercondylar notch of the femur. It limits posterior movement of the tibia on the femur (or anterior movement of the femur on the tibia). It takes the weight of the body when we are standing with our knees bent, or when we descend stairs or a slope. We can not easily manage without it.
Testing the ligaments
• Collateral ligaments. Take the leg in your hands and, keeping the knee straight, try (gently!) to abduct and adduct the knee. There should be little if any movement.
• Cruciates. Ask the patient to sit with the knees flexed to about a right angle. Sit on the foot of the side you are testing. Grasp the upper tibia in your hands and try to pull it forwards. If it comes forwards more than it should, the anterior cruciate is torn. Now push backwards. If the tibia goes back more than it should, the posterior cruciate is torn. Since someone (who?) imagined this to be similar to pulling and pushing a drawer open and closed, it is called the drawer test.
 |
| Fig. 13.17 |
Movements and muscles
Extension (Figs 13.8, 13.17)
Note: the tendon between the muscle and the patella is the quadriceps tendon; that from patella to tibia is the patellar ligament or tendon.
Knee jerk (patellar tendon reflex). Tapping the patellar tendon to elicit the knee jerk tests the femoral nerve and spinal segments L3, 4. It is an important part of a general neurological examination.
Flexion (Fig. 13.13)
Nerve supply: tibial nerve, L5–S3.
The hamstrings are attached to the ischial tuberosity above.




• Biceps femoris. This passes laterally to the head of the fibula. Its tendon is easily palpated as it approaches the fibula. Its long head comes from the ischial tuberosity, and its short head (supplied by the common fibular nerve) from the lower part of the linea aspera.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
