4
Abdomen
Arterial supply and venous drainage
Arterial supply to the gastrointestinal tract
Nervous system in the posterior abdominal region
Sympathetic trunks and splanchnic nerves
ADDITIONAL LEARNING RESOURCES FOR CHAPTER 4, ABDOMEN, ON STUDENT CONSULT (www.studentconsult.com)
 Image Library—illustrations of abdominal anatomy, Chapter 4
Image Library—illustrations of abdominal anatomy, Chapter 4
 Self-Assessment—National Board style multiple-choice questions, Chapter 4
Self-Assessment—National Board style multiple-choice questions, Chapter 4
 Short Questions—these are questions requiring short responses, Chapter 4
Short Questions—these are questions requiring short responses, Chapter 4
 Interactive Surface Anatomy—interactive surface animations, Chapter 4
Interactive Surface Anatomy—interactive surface animations, Chapter 4
 Medical Clinical Case Studies
Medical Clinical Case Studies Clinical Cases
Clinical CasesTraumatic rupture of the diaphragm
Chronic thrombosis of the inferior vena cava
Liver biopsy in patients with suspected liver cirrhosis
Complications of an abdominoperineal resection
Carcinoma of the head of the pancreas
Endoleak after endovascular repair of abdominal aortic aneurysm
Regional anatomy
The abdomen is the part of the trunk inferior to the thorax (Fig. 4.1). Its musculomembranous walls surround a large cavity (the abdominal cavity), which is bounded superiorly by the diaphragm and inferiorly by the pelvic inlet.
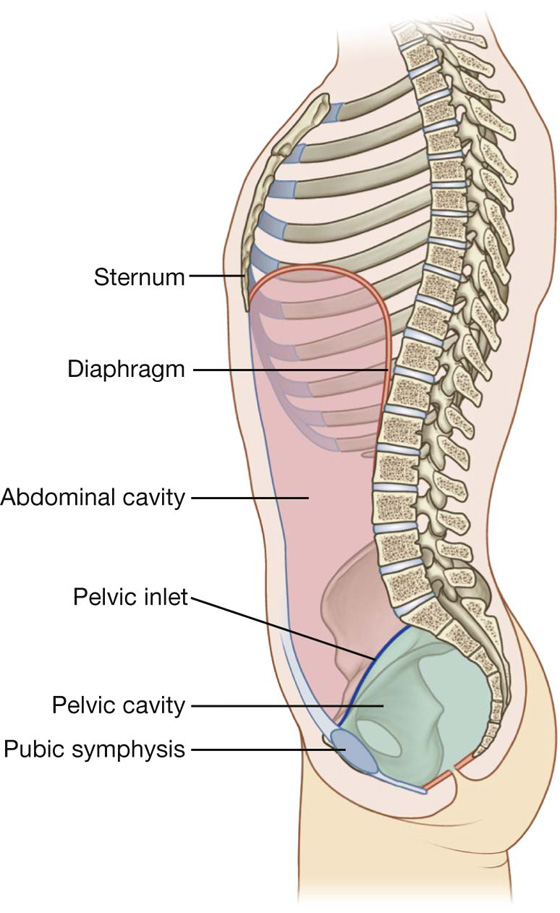
Fig. 4.1 Boundaries of the abdominal cavity.
The abdominal cavity may extend superiorly as high as the fourth intercostal space, and is continuous inferiorly with the pelvic cavity. It contains the peritoneal cavity and the abdominal viscera.
SURFACE TOPOGRAPHY
Topographical divisions of the abdomen are used to describe the location of abdominal organs and the pain associated with abdominal problems. The two schemes most often used are:
 a four-quadrant pattern, and
a four-quadrant pattern, and a nine-region pattern.
a nine-region pattern.Four-quadrant pattern
A horizontal transumbilical plane passing through the umbilicus and the intervertebral disc between vertebrae LIII and LIV and intersecting with the vertical median plane divides the abdomen into four quadrants—the right upper, left upper, right lower, and left lower quadrants (Fig. 4.2).
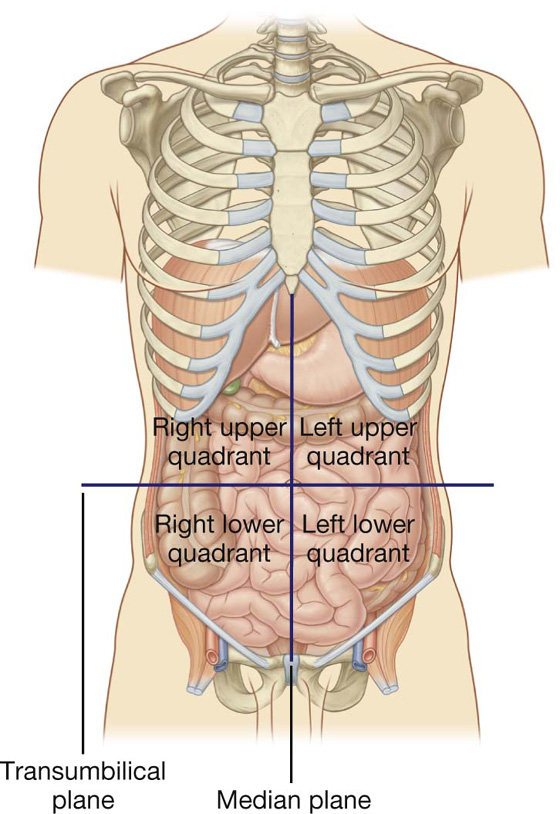
Fig. 4.2 Four-quadrant topographical pattern.
Nine-region pattern
The nine-region pattern is based on two horizontal and two vertical planes (Fig. 4.3).
 The superior horizontal plane (the subcostal plane) is immediately inferior to the costal margins, which places it at the lower border of the costal cartilage of rib X and passes posteriorly through the body of vertebra LIII. (Note, however, that sometimes the transpyloric plane, halfway between the jugular notch and the symphysis pubis or halfway between the umbilicus and the inferior end of the body of the sternum, passing posteriorly through the lower border of vertebrae LI and intersecting with the costal margin at the ends of the ninth costal cartilages, is used instead.)
The superior horizontal plane (the subcostal plane) is immediately inferior to the costal margins, which places it at the lower border of the costal cartilage of rib X and passes posteriorly through the body of vertebra LIII. (Note, however, that sometimes the transpyloric plane, halfway between the jugular notch and the symphysis pubis or halfway between the umbilicus and the inferior end of the body of the sternum, passing posteriorly through the lower border of vertebrae LI and intersecting with the costal margin at the ends of the ninth costal cartilages, is used instead.)
 The inferior horizontal plane (the intertubercular plane) connects the tubercles of the iliac crests, which are palpable structures 5 cm posterior to the anterior superior iliac spines, and passes through the upper part of the body of vertebra LV.
The inferior horizontal plane (the intertubercular plane) connects the tubercles of the iliac crests, which are palpable structures 5 cm posterior to the anterior superior iliac spines, and passes through the upper part of the body of vertebra LV. The vertical planes pass from the midpoint of the clavicles inferiorly to a point midway between the anterior superior iliac spine and pubic symphysis.
The vertical planes pass from the midpoint of the clavicles inferiorly to a point midway between the anterior superior iliac spine and pubic symphysis.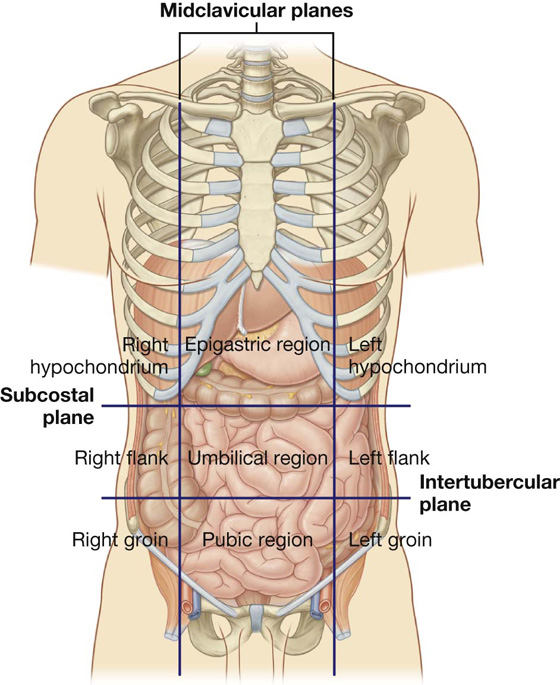
Fig. 4.3 Nine-region organizational pattern.
These four planes establish the topographical divisions in the nine-region organization. The following designations are used for each region: superiorly the right hypochondrium, the epigastric region, and the left hypochondrium; inferiorly the right groin (inguinal region), pubic region, and left groin (inguinal region); and in the middle the right flank (lateral region), the umbilical region, and the left flank (lateral region) (Fig. 4.3).
Surface anatomy
Using abdominal quadrants to locate major viscera
The abdomen can be divided into quadrants by a vertical median plane and a horizontal transumbilical plane (Fig. 4.4):
 The liver and gallbladder are in the right upper quadrant.
The liver and gallbladder are in the right upper quadrant.
 The stomach and spleen are in the left upper quadrant.
The stomach and spleen are in the left upper quadrant.
 The cecum and appendix are in the right lower quadrant.
The cecum and appendix are in the right lower quadrant.
 The end of the descending colon and sigmoid colon are in the left lower quadrant.
The end of the descending colon and sigmoid colon are in the left lower quadrant.
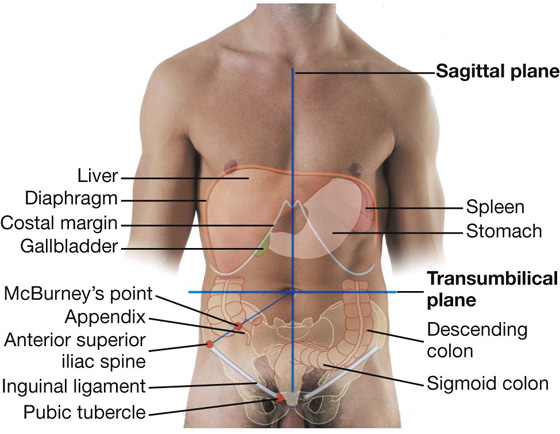
Fig. 4.4 Abdominal quadrants and the positions of major viscera. Anterior view of a man.
Most of the liver is under the right dome of the diaphragm and is deep to the lower thoracic wall. The inferior margin of the liver can be palpated descending below the right costal margin when a patient is asked to inhale deeply. On deep inspiration, the edge of the liver can be felt “slipping” under the palpating fingers placed under the costal margin.
A common surface projection of the appendix is McBurney’s point, which is one third of the way up a line from the right anterior superior iliac spine to the umbilicus.
Surface anatomy
Defining surface regions to which pain from the gut is referred
The abdomen can be divided into nine regions by a midclavicular sagittal plane on each side and by the subcostal and intertubercular planes, which pass through the body transversely (Fig. 4.5).
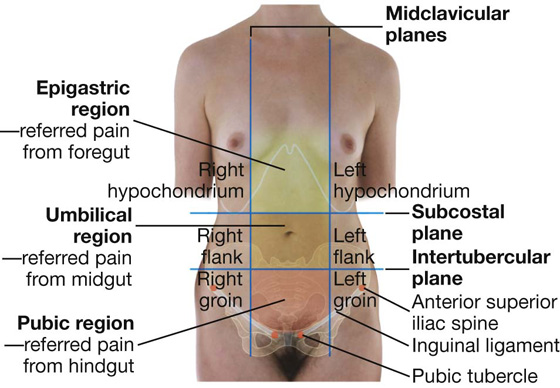
Fig. 4.5 The nine regions of the abdomen. Anterior view of a woman.
Pain from the abdominal part of the foregut is referred to the epigastric region, pain from the midgut is referred to the umbilical region, and pain from the hindgut is referred to the pubic region.
ABDOMINAL WALL
The abdominal wall covers a large area. It is bounded superiorly by the xiphoid process and costal margins, posteriorly by the vertebral column, and inferiorly by the upper parts of the pelvic bones.
Its layers consist of skin, superficial fascia (subcutaneous tissue), muscles and their associated deep fascias, extraperitoneal fascia, and parietal peritoneum (Fig. 4.6).
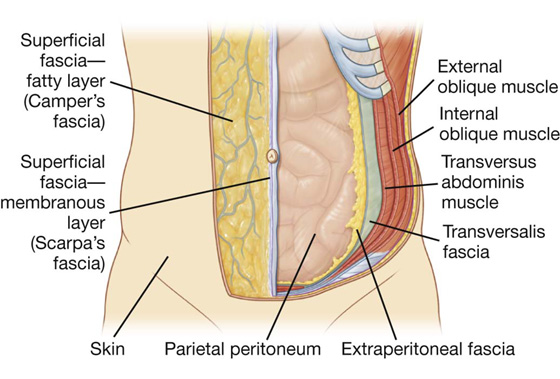
Fig. 4.6 Layers of the abdominal wall.
Superficial fascia
The superficial fascia of the abdominal wall (subcutaneous tissue of abdomen) is a layer of fatty connective tissue. It is usually a single layer similar to, and continuous with, the superficial fascia throughout other regions of the body. However, in the lower region of the anterior part of the abdominal wall, below the umbilicus, it forms two layers: a superficial fatty layer and a deeper membranous layer.
Superficial layer
The superficial fatty layer of superficial fascia (Camper’s fascia) contains fat and varies in thickness (Figs. 4.7, 4.8). It is continuous over the inguinal ligament with the superficial fascia of the thigh and with a similar layer in the perineum.
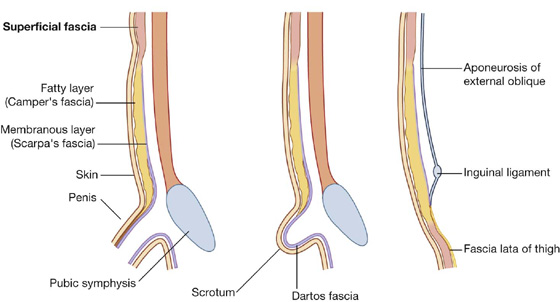
Fig. 4.7 Superficial fascia.
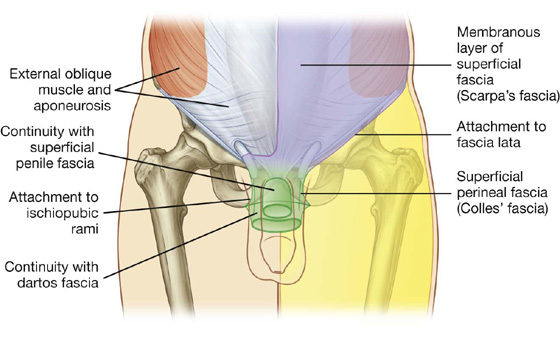
Fig. 4.8 Continuity of membranous layer of superficial fascia into other areas.
In men, this superficial layer continues over the penis and, after losing its fat and fusing with the deeper layer of superficial fascia, continues into the scrotum where it forms a specialized fascial layer containing smooth muscle fibers (the dartos fascia). In women, this superficial layer retains some fat and is a component of the labia majora.
Deeper layer
The deeper membranous layer of superficial fascia (Scarpa’s fascia) is thin and membranous, and contains little or no fat (Fig. 4.7). Inferiorly, it continues into the thigh, but just below the inguinal ligament, it fuses with the deep fascia of the thigh (the fascia lata; Fig. 4.8). In the midline, it is firmly attached to the linea alba and the pubic symphysis. It continues into the anterior part of the perineum where it is firmly attached to the ischiopubic rami and to the posterior margin of the perineal membrane. Here, it is referred to as the superficial perineal fascia (Colles’ fascia).
In men, the deeper membranous layer of superficial fascia blends with the superficial layer as they both pass over the penis, forming the superficial fascia of the penis, before they continue into the scrotum where they form the dartos fascia (Figs. 4.7, 4.8). Also in men, extensions of the deeper membranous layer of superficial fascia attached to the pubic symphysis pass inferiorly onto the dorsum and sides of the penis to form the fundiform ligament of the penis. In women, the membranous layer of the superficial fascia continues into the labia majora and the anterior part of the perineum.
Anterolateral muscles
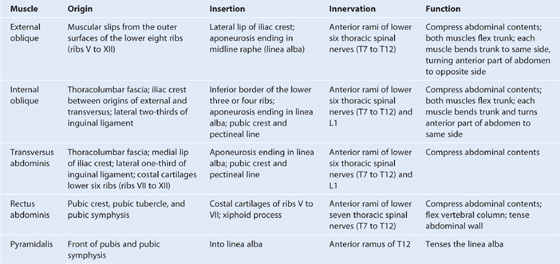
There are five muscles in the anterolateral group of abdominal wall muscles (Table 4.1):
 three flat muscles whose fibers begin posterolaterally, pass anteriorly, and are replaced by an aponeurosis as the muscle continues toward the midline—the external oblique, internal oblique, and transversus abdominis muscles;
three flat muscles whose fibers begin posterolaterally, pass anteriorly, and are replaced by an aponeurosis as the muscle continues toward the midline—the external oblique, internal oblique, and transversus abdominis muscles; two vertical muscles, near the midline, which are enclosed within a tendinous sheath formed by the aponeuroses of the flat muscles—the rectus abdominis and pyramidalis muscles.
two vertical muscles, near the midline, which are enclosed within a tendinous sheath formed by the aponeuroses of the flat muscles—the rectus abdominis and pyramidalis muscles.Table 4.1 Abdominal wall muscles
Each of these five muscles has specific actions, but together the muscles are critical:
 for the maintenance of many normal physiological functions,
for the maintenance of many normal physiological functions,
 to keep the abdominal viscera within the abdominal cavity,
to keep the abdominal viscera within the abdominal cavity,
 to protect the viscera from injury, and
to protect the viscera from injury, and
 to help maintain the position of the viscera in the erect posture against the action of gravity.
to help maintain the position of the viscera in the erect posture against the action of gravity.
Contraction of these muscles assists in both quiet and forced expiration by pushing the viscera upward (which helps push the relaxed diaphragm farther into the thoracic cavity) and in coughing and vomiting.
All these muscles are also involved in any action that increases intra-abdominal pressure, including parturition (childbirth), micturition (urination), and defecation (expulsion of feces from the rectum).
Flat muscles
External oblique
The most superficial of the three flat muscles in the anterolateral group of abdominal wall muscles is the external oblique, which is immediately deep to the superficial fascia (Table 4.1, Fig. 4.9). Its laterally placed muscle fibers pass in an inferomedial direction, while its large aponeurotic component covers the anterior part of the abdominal wall to the midline. Approaching the midline, the aponeuroses are entwined, forming the linea alba, which extends from the xiphoid process to the pubic symphysis.
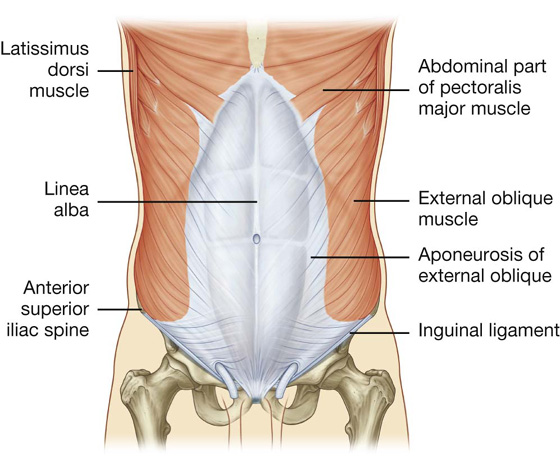
Fig. 4.9 External oblique muscle and its aponeurosis.
The lower border of the external oblique aponeurosis forms the inguinal ligament on each side (Fig. 4.9). This thickened reinforced free edge of the external oblique aponeurosis passes between the anterior superior iliac spine laterally and the pubic tubercle medially (Fig. 4.10). It folds under itself forming a trough, which plays an important role in the formation of the inguinal canal.
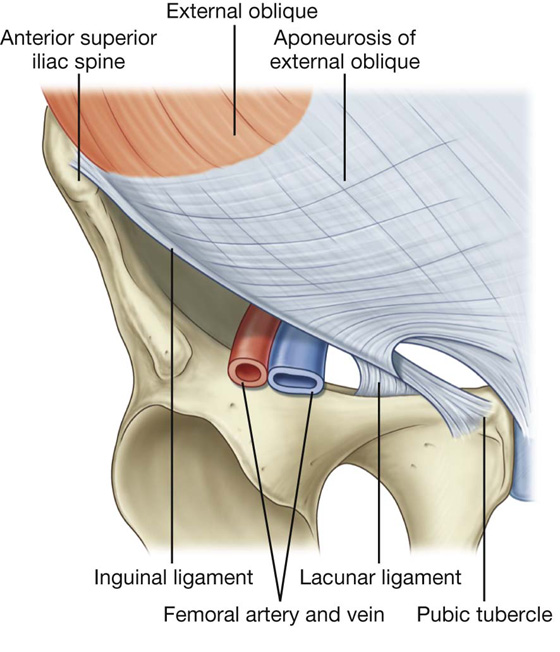
Fig. 4.10 Ligaments formed from the external oblique aponeurosis.
Several other ligaments are also formed from extensions of the fibers at the medial end of the inguinal ligament:
 The lacunar ligament is a crescent-shaped extension of fibers at the medial end of the inguinal ligament that pass backward to attach to the pecten pubis on the superior ramus of the pubic bone (Figs. 4.10, 4.11).
The lacunar ligament is a crescent-shaped extension of fibers at the medial end of the inguinal ligament that pass backward to attach to the pecten pubis on the superior ramus of the pubic bone (Figs. 4.10, 4.11).
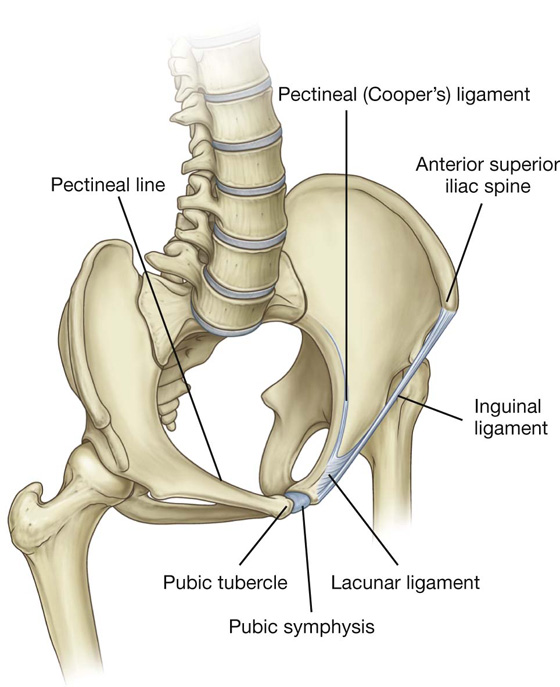
Fig. 4.11 Ligaments of the inguinal region.
 Additional fibers extend from the lacunar ligament along the pecten pubis of the pelvic brim to form the pectineal (Cooper’s) ligament.
Additional fibers extend from the lacunar ligament along the pecten pubis of the pelvic brim to form the pectineal (Cooper’s) ligament.Internal oblique
Deep to the external oblique muscle is the internal oblique muscle, which is the second of the three flat muscles (Table 4.1, Fig. 4.12). This muscle is smaller and thinner than the external oblique, with most of its muscle fibers passing in a superomedial direction. Its lateral muscular components end anteriorly as an aponeurosis that blends into the linea alba at the midline.
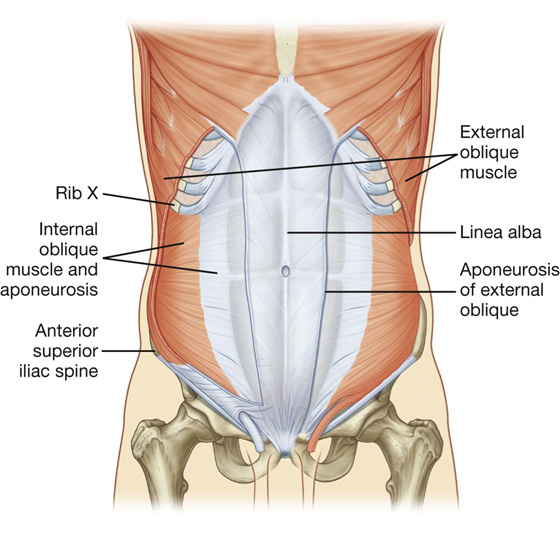
Fig. 4.12 Internal oblique muscle and its aponeurosis.
Transversus abdominis
Deep to the internal oblique muscle is the transversus abdominis muscle (Table 4.1, Fig. 4.13), so named because of the direction of most of its muscle fibers. It ends in an anterior aponeurosis, which blends with the linea alba at the midline.
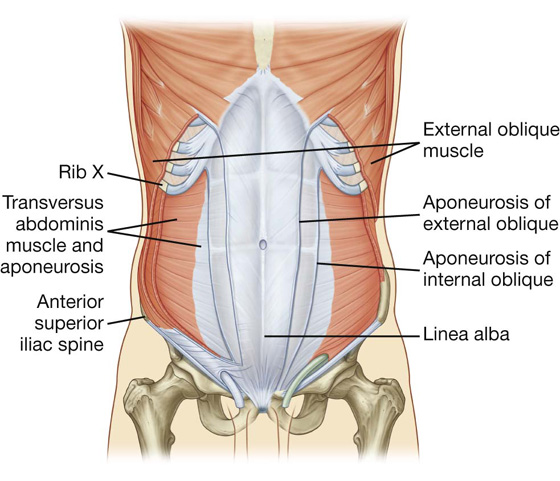
Fig. 4.13 Transversus abdominis muscle and its aponeurosis.
Transversalis fascia
Each of the three flat muscles is covered on its anterior and posterior surfaces by a layer of deep (or investing) fascia. In general, these layers are unremarkable except for the layer deep to the transversus abdominis muscle (the transversalis fascia), which is better developed.
The transversalis fascia is a continuous layer of deep fascia that lines the abdominal cavity and continues into the pelvic cavity. It crosses the midline anteriorly, associating with the transversalis fascia of the opposite side, and is continuous with the fascia on the inferior surface of the diaphragm. It is continuous posteriorly with the deep fascia covering the muscles of the posterior abdominal wall and attaches to the thoracolumbar fascia.
After attaching to the crest of the ilium, the transversalis fascia blends with the fascia covering the muscles associated with the upper regions of the pelvic bones and with similar fascia covering the muscles of the pelvic cavity. At this point, it is referred to as the parietal pelvic (or endopelvic) fascia.
There is therefore a continuous layer of deep fascia surrounding the abdominal cavity that is thick in some areas, thin in others, attached or free, and participates in the formation of specialized structures.
Vertical muscles
The two vertical muscles in the anterolateral group of abdominal wall muscles are the large rectus abdominis and the small pyramidalis (Table 4.1, Fig. 4.14).
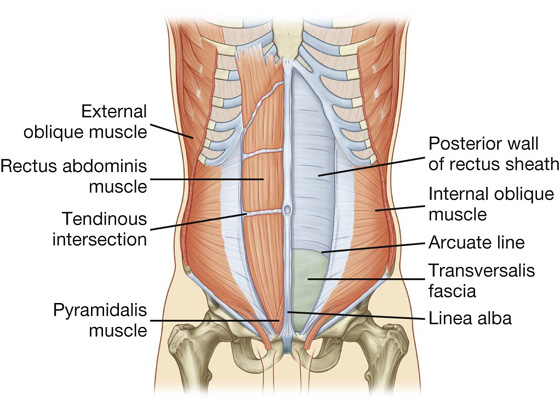
Fig. 4.14 Rectus abdominis and pyramidalis muscles.
Rectus abdominis
The rectus abdominis is a long, flat muscle and extends the length of the anterior abdominal wall. It is a paired muscle, separated in the midline by the linea alba, and it widens and thins as it ascends from the pubic symphysis to the costal margin. Along its course, it is intersected by three or four transverse fibrous bands or tendinous intersections (Fig. 4.14). These are easily visible on individuals with a well-developed rectus abdominis.
Pyramidalis
The second vertical muscle is the pyramidalis. This small, triangular muscle, which may be absent, is anterior to the rectus abdominis, has its base on the pubis, and its apex is attached superiorly and medially to the linea alba (Fig. 4.14).
Rectus sheath
The rectus abdominis and pyramidalis muscles are enclosed in an aponeurotic tendinous sheath (the rectus sheath) formed by a unique layering of the aponeuroses of the external and internal oblique, and transversus abdominis muscles (Fig. 4.15).
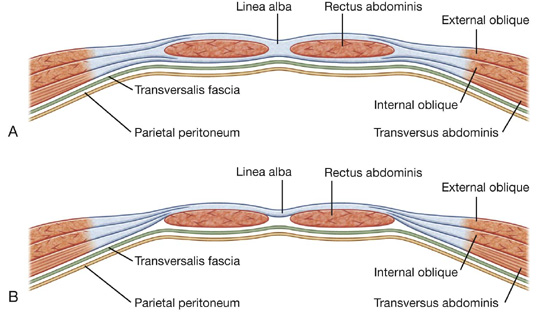
The rectus sheath completely encloses the upper three-quarters of the rectus abdominis and covers the anterior surface of the lower one-quarter of the muscle. As no sheath covers the posterior surface of the lower quarter of the rectus abdominis muscle, the muscle at this point is in direct contact with the transversalis fascia.
The formation of the rectus sheath surrounding the upper three-quarters of the rectus abdominis muscle has the following pattern:
 The anterior wall consists of the aponeurosis of the external oblique and half of the aponeurosis of the internal oblique, which splits at the lateral margin of the rectus abdominis.
The anterior wall consists of the aponeurosis of the external oblique and half of the aponeurosis of the internal oblique, which splits at the lateral margin of the rectus abdominis. The posterior wall of the rectus sheath consists of the other half of the aponeurosis of the internal oblique and the aponeurosis of the transversus abdominis.
The posterior wall of the rectus sheath consists of the other half of the aponeurosis of the internal oblique and the aponeurosis of the transversus abdominis.
At a point midway between the umbilicus and the pubic symphysis, corresponding to the beginning of the lower one-fourth of the rectus abdominis muscle, all of the aponeuroses move anterior to the rectus muscle. There is no posterior wall of the rectus sheath and the anterior wall of the sheath consists of the aponeuroses of the external oblique, the internal oblique, and the transversus abdominis muscles. From this point inferiorly, the rectus abdominis muscle is in direct contact with the transversalis fascia. Marking this point of transition is an arch of fibers (the arcuate line; see Fig. 4.14).
Extraperitoneal fascia
Deep to the transversalis fascia is a layer of connective tissue, the extraperitoneal fascia, which separates the transversalis fascia from the peritoneum (Fig. 4.16). Containing varying amounts of fat, this layer not only lines the abdominal cavity but is also continuous with a similar layer lining the pelvic cavity. It is abundant on the posterior abdominal wall, especially around the kidneys, continues over organs covered by peritoneal reflections, and, as the vasculature is located in this layer, extends into mesenteries with the blood vessels. Viscera in the extraperitoneal fascia are referred to as retroperitoneal.
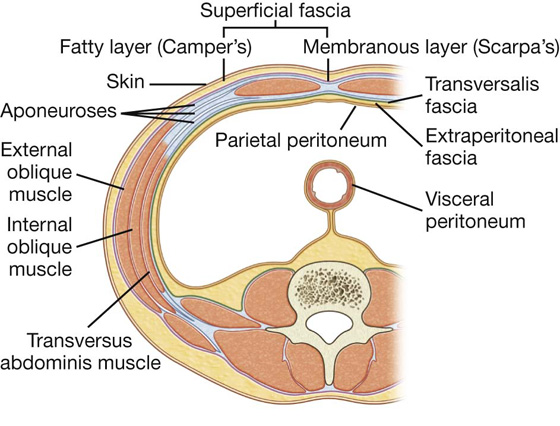
Fig. 4.16 Transverse section showing the layers of the abdominal wall.
Clinical app
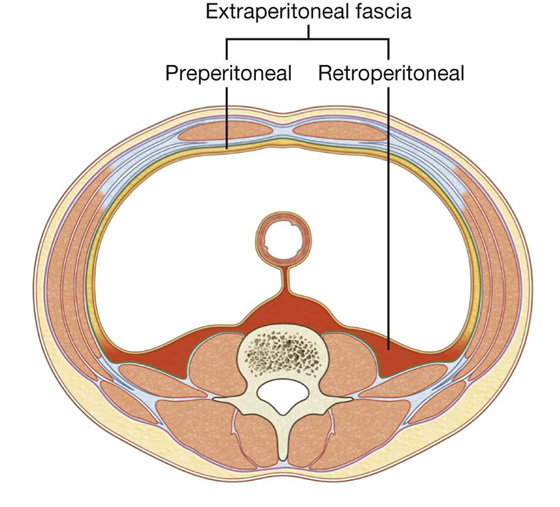
Preperitoneal vs. retroperitoneal
In the description of specific surgical procedures, the terminology used to describe the extraperitoneal fascia is further modified. The fascia toward the anterior side of the body is described as preperitoneal (or, less commonly, properitoneal, and the fascia toward the posterior side of the body has been described as retroperitoneal (Fig. 4.17). Examples of the use of these terms would be the continuity of fat in the inguinal canal with the preperitoneal fat and a transabdominal preperitoneal laparoscopic repair of an inguinal hernia.
Peritoneum
Deep to the extraperitoneal fascia is the peritoneum (Fig. 4.16). This thin serous membrane lines the walls of the abdominal cavity and, at various points, reflects onto the abdominal viscera, providing either a complete or a partial covering. The peritoneum lining the walls is the parietal peritoneum; the peritoneum covering the viscera is the visceral peritoneum.
The continuous lining of the abdominal walls by the parietal peritoneum forms a sac. This sac is closed in men, but has two openings in women where the uterine tubes provide a passage to the outside. The closed sac in men and the semiclosed sac in women is called the peritoneal cavity.
Innervation
The skin, muscles, and parietal peritoneum of the anterolateral abdominal wall are supplied by T7 to T12 and L1 spinal nerves. The anterior rami of these spinal nerves pass around the body, from posterior to anterior, in an inferomedial direction (Fig. 4.18). As they proceed, they give off a lateral cutaneous branch and end as an anterior cutaneous branch.
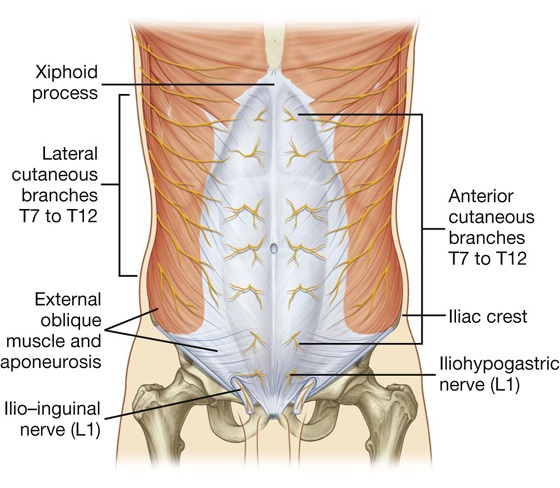
Fig. 4.18 Innervation of the anterolateral abdominal wall.
The intercostal nerves (T7 to T11) leave their intercostal spaces, passing deep to the costal cartilages, and continue onto the anterolateral abdominal wall between the internal oblique and transversus abdominis muscles (Fig. 4.19). Reaching the lateral edge of the rectus sheath, they enter the rectus sheath and pass posterior to the lateral aspect of the rectus abdominis muscle. Approaching the midline, an anterior cutaneous branch passes through the rectus abdominis muscle and the anterior wall of the rectus sheath to supply the skin.
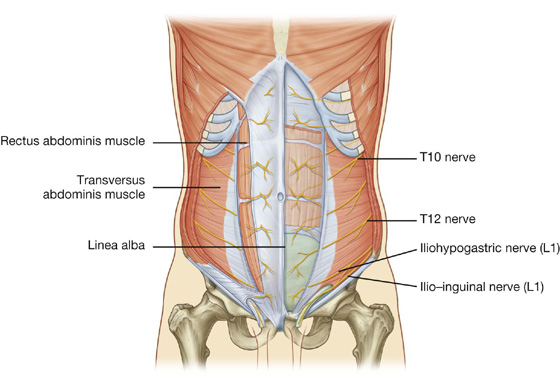
Fig. 4.19 Path taken by the nerves innervating the anterolateral abdominal wall.
Spinal nerve T12 (the subcostal nerve) follows a similar course as the intercostals. Branches of L1 (the iliohypogastric nerve and ilio-inguinal nerve), which originate from the lumbar plexus, follow similar courses initially, but deviate from this pattern near their final destination.
Along their course, nerves T7 to T12 and L1 supply branches to the anterolateral abdominal wall muscles and the underlying parietal peritoneum. All terminate by supplying skin (Fig. 4.20):
 Nerves T7 to T9 supply the skin from the xiphoid process to just above the umbilicus.
Nerves T7 to T9 supply the skin from the xiphoid process to just above the umbilicus.
 T10 supplies the skin around the umbilicus.
T10 supplies the skin around the umbilicus.
 T11, T12, and L1 supply the skin from just below the umbilicus to, and including, the pubic region.
T11, T12, and L1 supply the skin from just below the umbilicus to, and including, the pubic region.
 Additionally, the ilio-inguinal nerve (a branch of L1) supplies the anterior surface of the scrotum or labia majora, and sends a small cutaneous branch to the thigh.
Additionally, the ilio-inguinal nerve (a branch of L1) supplies the anterior surface of the scrotum or labia majora, and sends a small cutaneous branch to the thigh.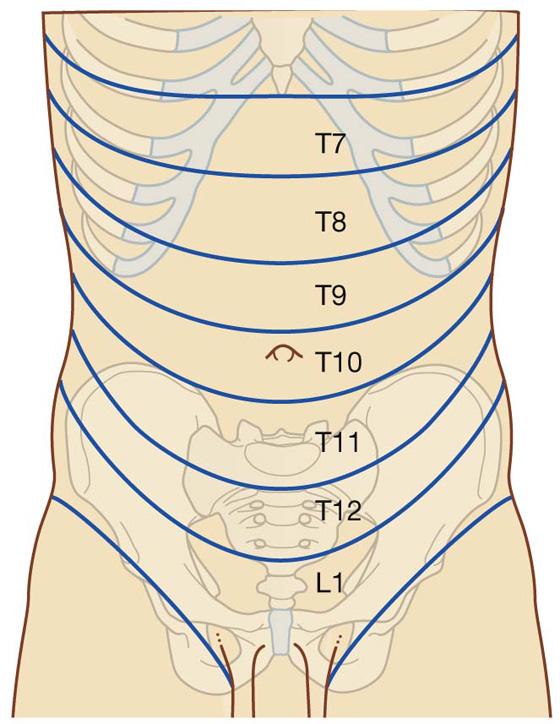
Fig. 4.20 Dermatomes of the anterolateral abdominal wall.
Arterial supply and venous drainage
Numerous blood vessels supply the anterolateral abdominal wall (Fig. 4.21). Superficially:
 The superior part of the wall is supplied by branches from the musculophrenic artery, a terminal branch of the internal thoracic artery.
The superior part of the wall is supplied by branches from the musculophrenic artery, a terminal branch of the internal thoracic artery. The inferior part of the wall is supplied by the medially placed superficial epigastric artery and the laterally placed superficial circumflex iliac artery, both branches of the femoral artery.
The inferior part of the wall is supplied by the medially placed superficial epigastric artery and the laterally placed superficial circumflex iliac artery, both branches of the femoral artery.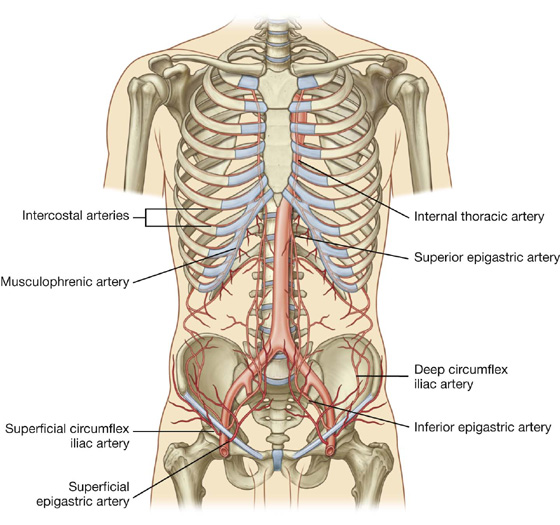
Fig. 4.21 Arterial supply to the anterolateral abdominal wall.
At a deeper level:
 The superior part of the wall is supplied by the superior epigastric artery, a terminal branch of the internal thoracic artery.
The superior part of the wall is supplied by the superior epigastric artery, a terminal branch of the internal thoracic artery. The lateral part of the wall is supplied by branches of the tenth and eleventh intercostal arteries and the subcostal artery.
The lateral part of the wall is supplied by branches of the tenth and eleventh intercostal arteries and the subcostal artery.
 The inferior part of the wall is supplied by the medially placed inferior epigastric artery and the laterally placed deep circumflex iliac artery, both branches of the external iliac artery.
The inferior part of the wall is supplied by the medially placed inferior epigastric artery and the laterally placed deep circumflex iliac artery, both branches of the external iliac artery.The superior and inferior epigastric arteries both enter the rectus sheath. They are posterior to the rectus abdominis muscle throughout their course, and anastomose with each other (Fig. 4.22).
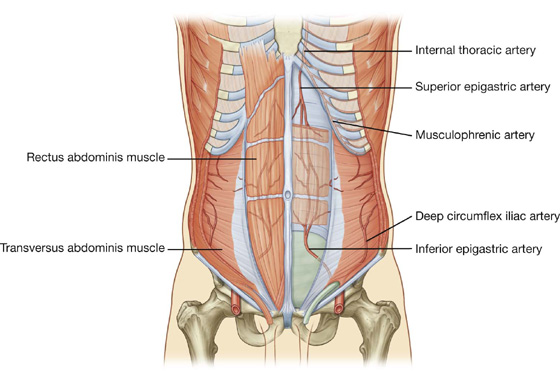
Fig. 4.22 Superior and inferior epigastric arteries.
Veins of similar names follow the arteries and are responsible for venous drainage.
Lymphatic drainage
Lymphatic drainage of the anterolateral abdominal wall follows the basic principles of lymphatic drainage:
 Superficial lymphatics above the umbilicus pass in a superior direction to the axillary nodes, while drainage below the umbilicus passes in an inferior direction to the superficial inguinal nodes.
Superficial lymphatics above the umbilicus pass in a superior direction to the axillary nodes, while drainage below the umbilicus passes in an inferior direction to the superficial inguinal nodes. Deep lymphatic drainage follows the deep arteries back to parasternal nodes along the internal thoracic artery, lumbar nodes along the abdominal aorta, and external iliac nodes along the external iliac artery.
Deep lymphatic drainage follows the deep arteries back to parasternal nodes along the internal thoracic artery, lumbar nodes along the abdominal aorta, and external iliac nodes along the external iliac artery.GROIN
The groin (inguinal region) is the area of junction between the anterior abdominal wall and the thigh. In this area, the abdominal wall is weakened from changes that occur during development and a peritoneal sac or diverticulum, with or without abdominal contents, can therefore protrude through it, creating an inguinal hernia. This type of hernia can occur in both sexes, but it is more common in males.
The inherent weakness in the anterior abdominal wall in the groin is caused by changes that occur during the development of the gonads. Before the descent of the testis and ovaries from their initial position high in the posterior abdominal wall, a peritoneal outpouching (the processus vaginalis) forms (Fig. 4.23), protruding through the various layers of the anterior abdominal wall and acquiring coverings from each:
 The transversalis fascia forms its deepest covering.
The transversalis fascia forms its deepest covering.
 The second covering is formed by the musculature of the internal oblique (a covering from the transversus abdominis muscle is not acquired because the processus vaginalis passes under the arching fibers of this abdominal wall muscle).
The second covering is formed by the musculature of the internal oblique (a covering from the transversus abdominis muscle is not acquired because the processus vaginalis passes under the arching fibers of this abdominal wall muscle). Its most superficial covering is the aponeurosis of the external oblique.
Its most superficial covering is the aponeurosis of the external oblique.
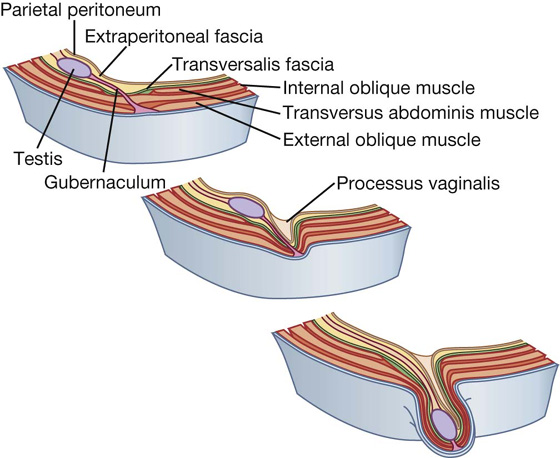
Fig. 4.23 Descent of the testes from week 7 (postfertilization) to birth.
The final event in this development is the descent of the testes into the scrotum or of the ovaries into the pelvic cavity. This process depends on the development of the gubernaculum (Fig. 4.23), which extends from the inferior border of the developing gonad to labioscrotal swellings in the developing perineum.
The processus vaginalis is immediately anterior to the gubernaculum within the inguinal canal.
In men, as the testes descend, the testes and their accompanying vessels, ducts, and nerves pass through the inguinal canal and are therefore surrounded by the same fascial layers of the abdominal wall. Testicular descent completes the formation of the spermatic cord in men.
In women, the ovaries descend into the pelvic cavity and become associated with the developing uterus. Therefore, the only remaining structure passing through the inguinal canal is the round ligament of the uterus, which is a remnant of the gubernaculum.
The development sequence is concluded in both sexes when the processus vaginalis obliterates. If this does not occur or is incomplete, a potential weakness exists in the anterior abdominal wall and an inguinal hernia may develop. In males, only proximal regions of the tunica vaginalis obliterate. The distal end expands to enclose most of the testes in the scrotum. In other words, the cavity of the tunica vaginalis in men forms as an extension of the developing peritoneal cavity that becomes separated off during development.
Inguinal canal
The inguinal canal is a slitlike passage that extends in a downward and medial direction, just above and parallel to the lower half of the inguinal ligament. It begins at the deep inguinal ring and continues for approximately 4 cm, ending at the superficial inguinal ring (Fig. 4.24). The contents of the canal are the genital branch of the genitofemoral nerve, the spermatic cord in men, and the round ligament of the uterus in women. Additionally, in both sexes, the ilio-inguinal nerve passes through part of the canal, exiting through the superficial inguinal ring with the other contents.
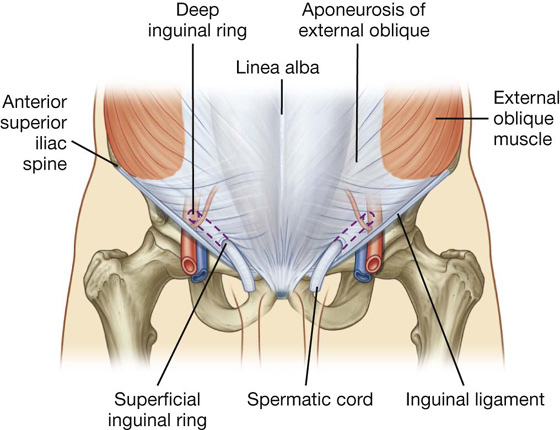
Fig. 4.24 Inguinal canal.
Deep inguinal ring
The deep (internal) inguinal ring is the beginning of the inguinal canal and is at a point midway between the anterior superior iliac spine and the pubic symphysis (Fig. 4.25). It is just above the inguinal ligament and immediately lateral to the inferior epigastric vessels. Although sometimes referred to as a defect or opening in the transversalis fascia, it is actually the beginning of the tubular evagination of transversalis fascia that forms one of the coverings (the internal spermatic fascia) of the spermatic cord in men or the round ligament of the uterus in women.
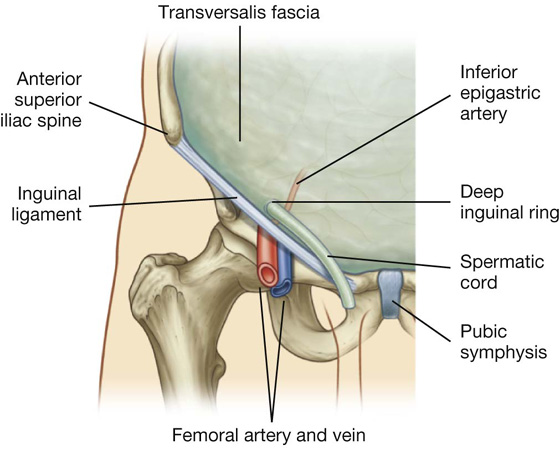
Fig. 4.25 Deep inguinal ring and the transversalis fascia.
Superficial inguinal ring
The superficial (external) inguinal ring is the end of the inguinal canal and is superior to the pubic tubercle (Fig. 4.26). It is a triangular opening in the aponeurosis of the external oblique, with its apex pointing superolaterally and its base formed by the pubic crest. The two remaining sides of the triangle (the medial crus and the lateral crus) are attached to the pubic symphysis and the pubic tubercle, respectively. At the apex of the triangle the two crura are held together by crossing (intercrural) fibers, which prevent further widening of the superficial ring.
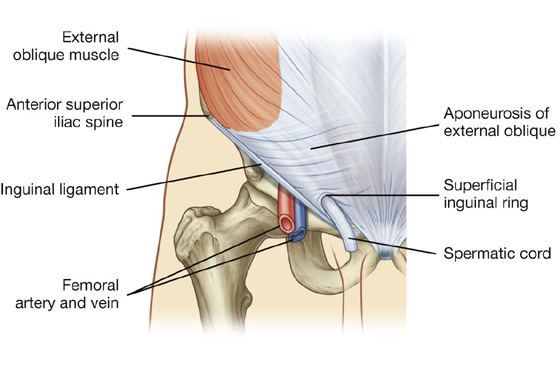
Fig. 4.26 Superficial inguinal ring and the aponeurosis of the external oblique.
As with the deep inguinal ring, the superficial inguinal ring is actually the beginning of the tubular evagination of the aponeurosis of the external oblique onto the structures traversing the inguinal canal and emerging from the superficial inguinal ring. This continuation of tissue over the spermatic cord is the external spermatic fascia.
Anterior wall
The anterior wall of the inguinal canal is formed along its entire length by the aponeurosis of the external oblique muscle (Fig. 4.26). It is also reinforced laterally by the lower fibers of the internal oblique that originate from the lateral two-thirds of the inguinal ligament (Fig. 4.27). This adds an additional covering over the deep inguinal ring, which is a potential point of weakness in the anterior abdominal wall. Furthermore, as the internal oblique muscle covers the deep inguinal ring, it also contributes a layer (the cremasteric fascia containing the cremasteric muscle) to the coverings of the structures traversing the inguinal canal.
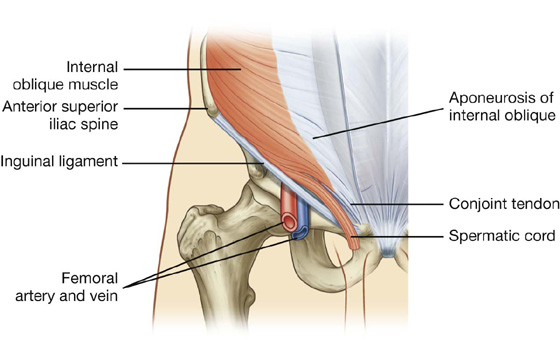
Fig. 4.27 Internal oblique muscle and the inguinal canal.
Posterior wall
The posterior wall of the inguinal canal is formed along its entire length by the transversalis fascia (see Fig. 4.25). It is reinforced along its medial one-third by the conjoint tendon (inguinal falx; Fig. 4.27). This tendon is the combined insertion of the transversus abdominis and internal oblique muscles into the pubic crest and pectineal line.
As with the internal oblique muscle’s reinforcement of the area of the deep inguinal ring, the position of the conjoint tendon posterior to the superficial inguinal ring provides additional support to a potential point of weakness in the anterior abdominal wall.
Roof
The roof (superior wall) of the inguinal canal is formed by the arching fibers of the transversus abdominis and internal oblique muscles (Figs. 4.27, 4.28). They pass from their lateral points of origin from the inguinal ligament to their common medial attachment as the conjoint tendon.

Fig. 4.28 Transversus abdominis muscle and the inguinal canal.
Floor
The floor (inferior wall) of the inguinal canal is formed by the medial one-half of the inguinal ligament. This rolled-under, free margin of the lowest part of the aponeurosis of the external oblique forms a gutter or trough on which the contents of the inguinal canal are positioned. The lacunar ligament reinforces most of the medial part of the gutter.
Contents
The contents of the inguinal canal are:
 the spermatic cord in men,
the spermatic cord in men, the round ligament of the uterus, and
the round ligament of the uterus, and
 genital branch of the genitofemoral nerve in women.
genital branch of the genitofemoral nerve in women.
These structures enter the inguinal canal through the deep inguinal ring and exit it through the superficial inguinal ring.
Additionally, the ilio-inguinal nerve (L1) passes through part of the inguinal canal. This nerve is a branch of the lumbar plexus, and enters the abdominal wall posteriorly by piercing the internal surface of the transversus abdominis muscle and continues through the layers of the anterior abdominal wall by piercing the internal oblique muscle. As it continues to pass inferomedially, it enters the inguinal canal. It continues down the canal to exit through the superficial inguinal ring.
Spermatic cord
The spermatic cord begins to form proximally at the deep inguinal ring and consists of structures passing between the abdominopelvic cavities and the testes, and the three fascial coverings that enclose these structures (Fig. 4.29).
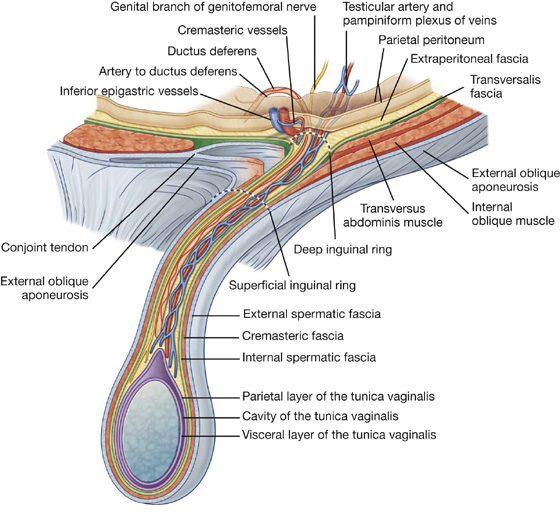
Fig. 4.29 Spermatic cord.
The structures in the spermatic cord include:
 the ductus deferens,
the ductus deferens, the artery to ductus deferens (from the inferior vesical artery),
the artery to ductus deferens (from the inferior vesical artery),
 the testicular artery (from the abdominal aorta),
the testicular artery (from the abdominal aorta),
 the pampiniform plexus of veins (testicular veins),
the pampiniform plexus of veins (testicular veins),
 the cremasteric artery and vein (small vessels associated with the cremasteric fascia),
the cremasteric artery and vein (small vessels associated with the cremasteric fascia),
 the genital branch of the genitofemoral nerve (innervation to the cremasteric muscle),
the genital branch of the genitofemoral nerve (innervation to the cremasteric muscle),
 sympathetic and visceral afferent nerve fibers,
sympathetic and visceral afferent nerve fibers,
 lymphatics, and
lymphatics, and remnants of the processus vaginalis.
remnants of the processus vaginalis.
These structures enter the deep inguinal ring, proceed down the inguinal canal, and exit from the superficial inguinal ring, having acquired the three fascial coverings during their journey. This collection of structures and fascias continues into the scrotum, where the structures connect with the testes and the fascias surround the testes.
The fascias enclosing the contents of the spermatic cord include (Fig. 4.29):
 the internal spermatic fascia, which is the deepest layer, arises from the transversalis fascia, and is attached to the margins of the deep inguinal ring;
the internal spermatic fascia, which is the deepest layer, arises from the transversalis fascia, and is attached to the margins of the deep inguinal ring;
 the cremasteric fascia with the associated cremasteric muscle, which is the middle fascial layer and arises from the internal oblique muscle; and
the cremasteric fascia with the associated cremasteric muscle, which is the middle fascial layer and arises from the internal oblique muscle; and the external spermatic fascia, which is the most superficial covering of the spermatic cord, arises from the aponeurosis of the external oblique muscle, and is attached to the margins of the superficial inguinal ring (Fig. 4.29).
the external spermatic fascia, which is the most superficial covering of the spermatic cord, arises from the aponeurosis of the external oblique muscle, and is attached to the margins of the superficial inguinal ring (Fig. 4.29).
Round ligament of the uterus
The round ligament of the uterus is a cordlike structure that passes from the uterus to the deep inguinal ring where it enters the inguinal canal. It passes down the inguinal canal and exits through the superficial inguinal ring. At this point, it has changed from a cordlike structure to a few strands of tissue, which attach to the connective tissue associated with the labia majora. As it traverses the inguinal canal, it acquires the same coverings as the spermatic cord in men.
The round ligament of the uterus is the long distal part of the original gubernaculum in the fetus that extends from the ovary to the labioscrotal swellings. From its attachment to the uterus, the round ligament of the uterus continues to the ovary as the ligament of the ovary that develops from the short proximal end of the gubernaculum.
Clinical app
Surgical incisions
Traditionally, incisions have been placed at and around the region of surgical interest. The size of these incisions was usually large to allow good access and optimal visualization of the abdominal cavity.
Currently, the most commonly used large abdominal incision is a central craniocaudad incision from the xiphoid process to the pubic symphysis, which provides wide access to the whole of the abdominal contents and allows an exploratory procedure to be performed (laparotomy).
With the advent of small cameras and the development of minimal access surgery, tiny incisions can be made in the anterior abdominal wall and cameras inserted. The peritoneal cavity is “inflated” with carbon dioxide to increase the space in which the procedure is performed. Further instruments may be inserted through small portholes, and procedures such as cholecystectomy (removal of the gallbladder) and appendectomy (removal of the appendix) can be carried out, allowing the patient to return home sooner.
Surface anatomy
How to find the superficial inguinal ring
The superficial inguinal ring is superior to the pubic crest and tubercle and to the medial end of the inguinal ligament (Fig. 4.30):
 In men, the superficial inguinal ring can be easily located by following the spermatic cord superiorly to the lower abdominal wall—the external spermatic fascia of the spermatic cord is continuous with the margins of the superficial inguinal ring.
In men, the superficial inguinal ring can be easily located by following the spermatic cord superiorly to the lower abdominal wall—the external spermatic fascia of the spermatic cord is continuous with the margins of the superficial inguinal ring. In women, the pubic tubercle can be palpated and the ring is superior and lateral to it.
In women, the pubic tubercle can be palpated and the ring is superior and lateral to it.
 The deep inguinal ring, which is the internal opening to the inguinal canal, lies superior to the inguinal ligament, midway between the anterior superior iliac spine and pubic symphysis. The pulse of the femoral artery can be felt in the same position, but below the inguinal ligament.
The deep inguinal ring, which is the internal opening to the inguinal canal, lies superior to the inguinal ligament, midway between the anterior superior iliac spine and pubic symphysis. The pulse of the femoral artery can be felt in the same position, but below the inguinal ligament.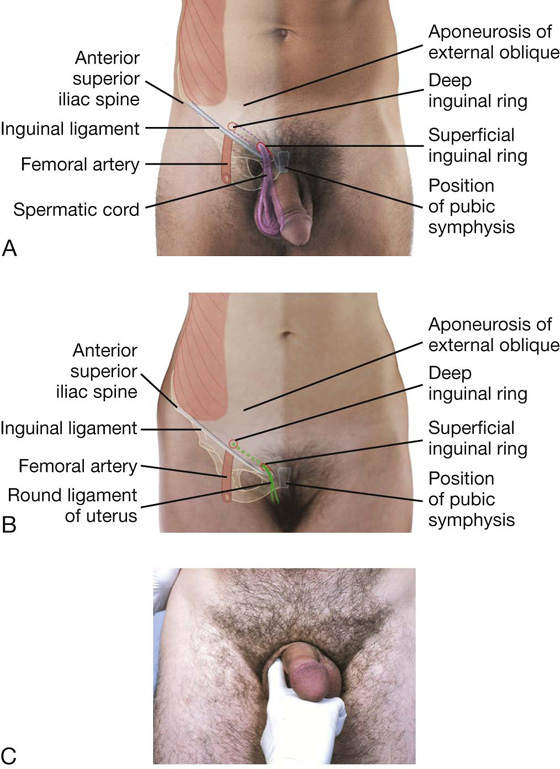
Because the superficial inguinal ring is the site where inguinal hernias appear, particularly in men, the ring and related parts of the inguinal canal are often evaluated during physical examination.
Clinical app
Cremasteric reflex
In men, the cremaster muscle and cremasteric fascia form the middle or second covering of the spermatic cord. This muscle and its associated fascia are supplied by the genital branch of the genitofemoral nerve (L1/L2). Contraction of this muscle can be stimulated by a reflex arc. Gentle touch at and around the skin of the medial aspect of the superior part of the thigh stimulates the sensory fibers in the ilio-inguinal nerve. These sensory fibers enter the spinal cord at level L1. At this level, the sensory fibers stimulate the motor fibers carried in the genital branch of the genitofemoral nerve and the testis elevates on the stimulated side.
Clinical app
Masses around the groin
The most common masses in the groin are hernias. A hernia is the protrusion of a viscus, in part or in whole, through a normal or abnormal opening. The viscus usually carries a covering of parietal peritoneum, which forms the lining of the hernial sac.
The key to groin examination is determining the position of the inguinal ligament. The inguinal ligament passes between the anterior superior iliac spine laterally and the pubic tubercle medially. Inguinal hernias are above the inguinal ligament and are usually more apparent on standing. A visual assessment of the lump is necessary, bearing in mind the anatomical landmarks of the inguinal ligament.
In men, it is wise to examine the scrotum to check for a lump. If an abnormal mass is present, an inability to feel its upper edge suggests that it may originate from the inguinal canal and might be a hernia. By placing the hand over the lump and asking the patient to cough, the lump bulges outward.
An attempt should be made to reduce the swelling by applying gentle, firm pressure over the lump. If the lump is reducible, the hand should be withdrawn and careful observation will reveal recurrence of the mass.
The position of an abnormal mass in the groin relative to the pubic tubercle is very important, as are the presence of increased temperature and pain, which may represent early signs of strangulation or infection.
As a general rule:
 An inguinal hernia appears through the superficial inguinal ring above the pubic tubercle and crest.
An inguinal hernia appears through the superficial inguinal ring above the pubic tubercle and crest.
 A femoral hernia appears through the femoral canal below and lateral to the pubic tubercle.
A femoral hernia appears through the femoral canal below and lateral to the pubic tubercle.
Clinical app
Inguinal hernias
An inguinal hernia is the protrusion or passage of a peritoneal sac, with or without abdominal contents, through a weakened part of the abdominal wall in the groin. It occurs because the peritoneal sac enters the inguinal canal either:
 indirectly, through the deep inguinal ring, or
indirectly, through the deep inguinal ring, or
 directly, through the posterior wall of the inguinal canal.
directly, through the posterior wall of the inguinal canal.
 Inguinal hernias are therefore classified as either indirect or direct and occur more commonly in men than in women possibly because men have a much larger inguinal canal than women.
Inguinal hernias are therefore classified as either indirect or direct and occur more commonly in men than in women possibly because men have a much larger inguinal canal than women.Clinical app
Indirect inguinal hernias
The indirect inguinal hernia is the most common of the two types of inguinal hernias and is much more common in men than in women (Fig. 4.31). It usually occurs because some part, or all, of the embryonic processus vaginalis remains open or patent. It is therefore referred to as being congenital in origin.
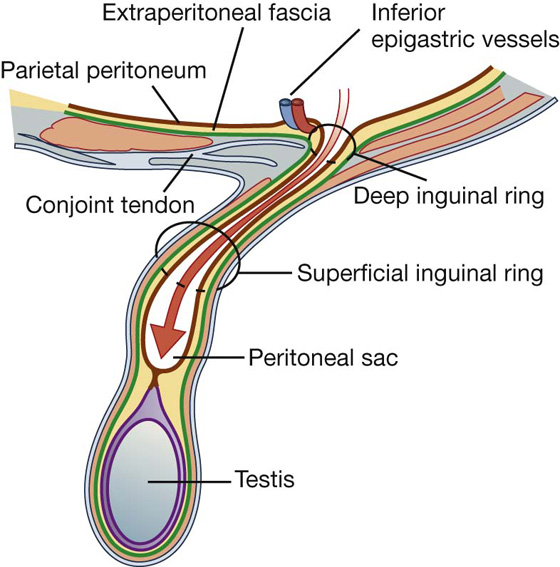
Fig. 4.31 Indirect inguinal hernia.
The protruding peritoneal sac enters the inguinal canal by passing through the deep inguinal ring, just lateral to the inferior epigastric vessels. The extent of its excursion down the inguinal canal depends on the amount of processus vaginalis that remains patent. If the entire processus vaginalis remains patent, the peritoneal sac may traverse the length of the canal, exit the superficial inguinal ring, and continue into the scrotum in men or the labia majus in women. In this case, the protruding peritoneal sac acquires the same coverings as those associated with the spermatic cord in men or the round ligament of the uterus in women.
Clinical app
Direct inguinal hernias
A peritoneal sac that enters the medial end of the inguinal canal directly through a weakened posterior wall is a direct inguinal hernia (Fig. 4.32). It is usually described as acquired because it develops when abdominal musculature has been weakened and is commonly seen in mature men.
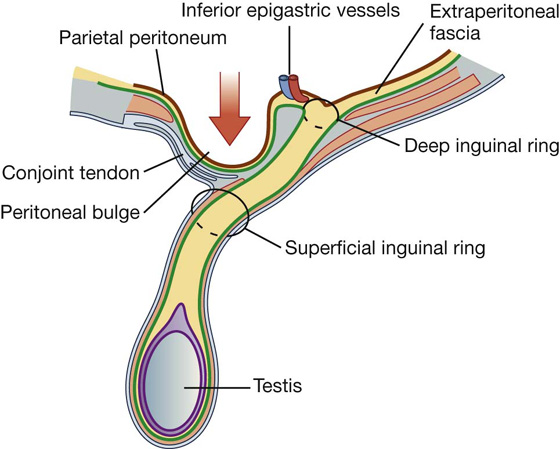
Fig. 4.32 Direct inguinal hernia.
This type of inguinal hernia does not traverse the entire length of the inguinal canal, but may exit through the superficial inguinal ring. When this occurs, the peritoneal sac acquires a layer of external spermatic fascia and can extend, like an indirect hernia, into the scrotum. Also, unlike indirect inguinal hernias that originate lateral to the inferior epigastric artery, direct inguinal hernias originate medial to the artery (Fig. 4.32).
Femoral hernias
A femoral hernia passes through the femoral canal and into the medial aspect of the anterior thigh. The femoral canal lies at the medial edge of the femoral sheath, which contains the femoral artery, femoral vein, and lymphatics. The neck of the femoral canal is extremely narrow and is prone to trapping bowel within the sac, making this type of hernia irreducible and susceptible to bowel strangulation. Femoral hernias are usually acquired, and most commonly occur in middle-aged and elderly populations. In addition, because women generally have wider pelvises than men, they tend to occur more commonly in women.
Clinical app
Umbilical hernias
Umbilical hernias are rare. Occasionally, they are congenital and result from failure of the small bowel to return to the abdominal cavity from the umbilical cord during development. After birth, umbilical hernias may result from incomplete closure of the umbilicus (navel). Overall, most of these hernias close in the first year of life, and surgical repair is not generally attempted until later.
Para-umbilical hernias may occur in adults at and around the umbilicus and often have small necks, so requiring surgical treatment.
Clinical app
Incisional hernias
Incisional hernias occur through a defect in a scar of a previous abdominal operation. Usually, the necks of these hernias are wide and do not therefore strangulate the viscera they contain.
Clinical app
Sportsmen’s groin/sportsmen’s hernia
The groin can loosely be defined as the area where the leg meets the trunk near the midline. Here the abdominal muscles of the trunk blend in with the adductor muscles of the thigh, the medial end of the inguinal ligament attaches to the pubic tubercle, the pubic symphysis attaches the two pubic bones together, and the superficial (external) inguinal ring occurs. It also is in and around this region where there is considerable translation of force during most athletic and sporting activities. Pain in the groin or pubic region can be due to numerous causes, which include inflammatory changes at the pubic symphysis, insertional problems of the rectus abdominus/adductor longus, and hernias.
Clinical app
Other hernias
A spigelian hernia passes upward through the arcuate line into the lateral border at the lower part of the posterior rectus sheath. It may appear as a tender mass on one side of the lower anterior abdominal wall.
Abdominopelvic cavity hernias can also develop in association with the pelvic walls, and sites include the obturator canal, the greater sciatic foramen, above and below the piriformis muscle.
Clinical app
Potential problem of hernias
One of the potential problems with hernias is that bowel and fat may become stuck within the hernial sac. This can cause appreciable pain and bowel obstruction, necessitating urgent surgery. Another potential risk is strangulation of the hernia, in which the blood supply to the bowel is cut off at the neck of the hernial sac, rendering the bowel ischemic and susceptible to perforation.
ABDOMINAL VISCERA
Peritoneum
A thin membrane (the peritoneum) lines the walls of the abdominal cavity and covers much of the viscera. The parietal peritoneum lines the walls of the cavity and the visceral peritoneum covers the viscera. Between the parietal and visceral layers of peritoneum is a potential space (the peritoneal cavity). Abdominal viscera either are suspended in the peritoneal cavity by folds of peritoneum (mesenteries) or are outside the peritoneal cavity. Organs suspended in the cavity are referred to as intraperitoneal (Fig. 4.33); organs outside the peritoneal cavity, with only one surface or part of one surface covered by peritoneum, are retroperitoneal.
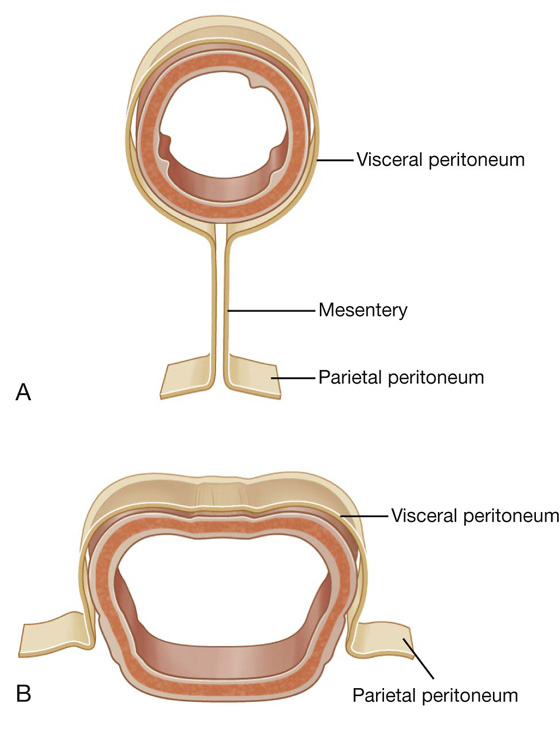
Fig. 4.33 A. Intraperitoneal. B. Retroperitoneal.
Peritoneal cavity
The peritoneal cavity is subdivided into the greater sac and the omental bursa (lesser sac; Fig. 4.34).
 The greater sac accounts for most of the space in the peritoneal cavity, beginning superiorly at the diaphragm and continuing inferiorly into the pelvic cavity. It is entered once the parietal peritoneum has been penetrated.
The greater sac accounts for most of the space in the peritoneal cavity, beginning superiorly at the diaphragm and continuing inferiorly into the pelvic cavity. It is entered once the parietal peritoneum has been penetrated. The omental bursa is a smaller subdivision of the peritoneal cavity posterior to the stomach and liver and is continuous with the greater sac through an opening, the omental (epiploic) foramen (Fig. 4.35).
The omental bursa is a smaller subdivision of the peritoneal cavity posterior to the stomach and liver and is continuous with the greater sac through an opening, the omental (epiploic) foramen (Fig. 4.35).
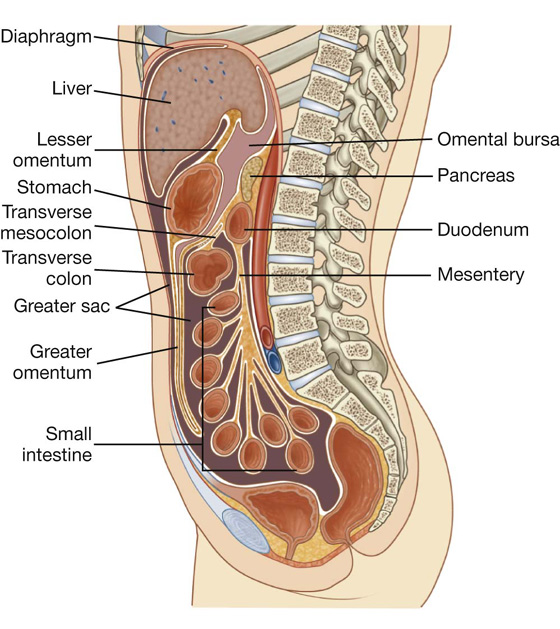
Fig. 4.34 Greater and lesser sacs of the peritoneal cavity.
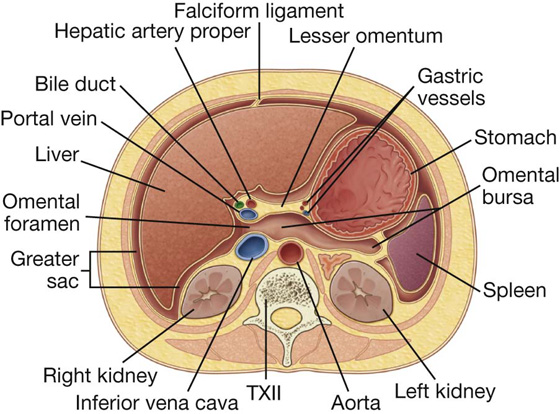
Surrounding the omental (epiploic) foramen are numerous structures covered with peritoneum (Fig. 4.35). They include the portal vein, hepatic artery proper, and bile duct anteriorly; the inferior vena cava posteriorly; the caudate lobe of the liver superiorly; and the first part of the duodenum inferiorly.
Clinical app
The peritoneum
The peritoneum has a large surface area, which facilitates the spread of disease through the peritoneal cavity and over the bowel and visceral surfaces. Conversely, this large surface area can be used for administering certain types of treatment and a number of procedures.
Clinical app
Innervation of peritoneum
The parietal peritoneum associated with the abdominal wall is innervated by somatic afferents carried in branches of the associated spinal nerves and is therefore sensitive to well-localized pain. The visceral peritoneum is innervated by visceral afferents that accompany autonomic nerves (sympathetic and parasympathetic) back to the central nervous system. Activation of these fibers can lead to referred pain and poorly localized sensations of discomfort, and to reflex visceral motor activity.
Clinical app
Ventriculoperitoneal shunts
Patients with obstructive hydrocephalus (an excessive accumulation of cerebrospinal fluid within the cerebral ventricular system) require continuous drainage of this fluid. This is achieved by placing a catheter through the skull into the cerebral ventricles and placing the extracranial part of the tube beneath the scalp and skin of the chest wall and then passing it through the abdominal wall into the peritoneal cavity. Cerebrospinal fluid drains through the tube into the peritoneal cavity where it is absorbed.
Dialysis and peritoneal dialysis
People who develop renal failure require dialysis to live. There are two methods.
In the first method (hemodialysis), blood is taken from the circulation, dialyzed through a complex artificial membrane, and returned to the body. A high rate of blood flow is required to remove excess body fluid, exchange electrolytes, and remove noxious metabolites. To accomplish this, either an arteriovenous fistula is established surgically and is cannulated each time the patient returns for dialysis, or a large-bore cannula is placed into the right atrium, through which blood can be aspirated and returned.
In the second method of dialysis, the peritoneum is used as the dialysis membrane. The large surface area of the peritoneal cavity is an ideal dialysis membrane for fluid and electrolyte exchange. To accomplish dialysis, a small tube is inserted through the abdominal wall and dialysis fluid is injected into the peritoneal cavity. Electrolytes and molecules are exchanged across the peritoneum between the fluid and blood. Once dialysis is completed, the fluid is drained.
Clinical app
Peritoneal spread of disease
The large surface area of the peritoneal cavity allows infection and malignant disease to spread easily throughout the abdomen. If malignant cells enter the peritoneal cavity by direct invasion (e.g., from colon or ovarian cancer), spread may be rapid. Similarly, a surgeon excising a malignant tumor and releasing malignant cells into the peritoneal cavity may cause an appreciable worsening of the patient’s prognosis.
Clinical app
Perforated bowel
A perforated bowel (e.g., caused by a perforated duodenal ulcer) often leads to the release of gas into the peritoneal cavity. This peritoneal gas can be easily visualized on a chest radiograph, with the patient standing, where gas can be demonstrated in extremely small amounts beneath the diaphragm. A patient with severe abdominal pain and subdiaphragmatic gas needs a laparotomy.
Omenta, mesenteries, and ligaments
Throughout the peritoneal cavity, numerous peritoneal folds connect organs to each other or to the abdominal wall. These folds (omenta, mesenteries, and ligaments) develop from the original dorsal and ventral mesenteries, which suspend the developing gastrointestinal tract in the embryonic coelomic cavity. Some contain vessels and nerves supplying the viscera, whereas others help maintain the proper positioning of the viscera.
Omenta
The omenta consist of two layers of peritoneum, which pass from the stomach and the first part of the duodenum to other viscera. There are two:
 the greater omentum derived from the dorsal mesentery, and
the greater omentum derived from the dorsal mesentery, and
 the lesser omentum derived from the ventral mesentery.
the lesser omentum derived from the ventral mesentery.
The greater omentum is a large, apron-like, peritoneal fold that attaches to the greater curvature of the stomach and the first part of the duodenum (Fig. 4.36). It drapes inferiorly over the transverse colon and the coils of the jejunum and ileum (see Fig. 4.34). Turning posteriorly, it ascends to associate with, and become adherent to, the peritoneum on the superior surface of the transverse colon and the anterior layer of the transverse mesocolon before arriving at the posterior abdominal wall.
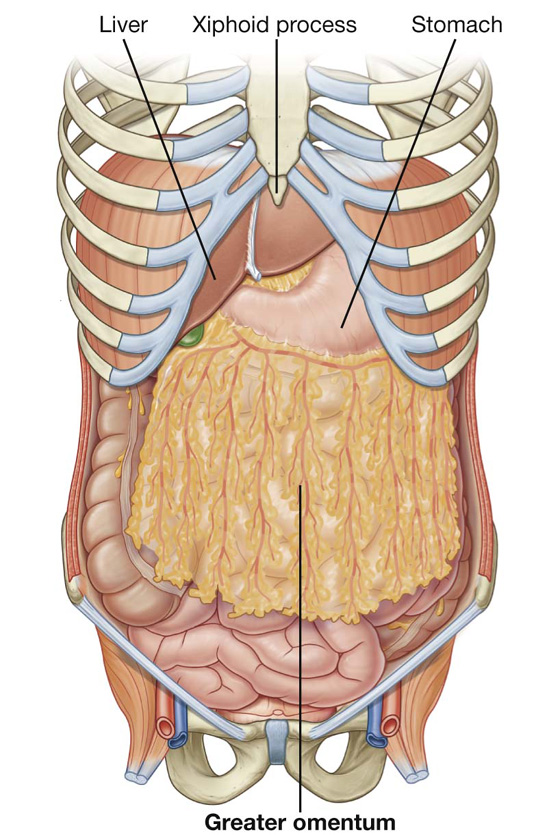
Fig. 4.36 Greater omentum.
Usually a thin membrane, the greater omentum always contains an accumulation of fat, which may become substantial in some individuals. Additionally, there are two arteries and accompanying veins, the right and left gastro-omental vessels, between this double-layered peritoneal apron just inferior to the greater curvature of the stomach.
The other two-layered peritoneal omentum is the lesser omentum (Fig. 4.37). It extends from the lesser curvature of the stomach and the first part of the duodenum to the inferior surface of the liver (Fig. 4.37; also see Fig. 4.34).
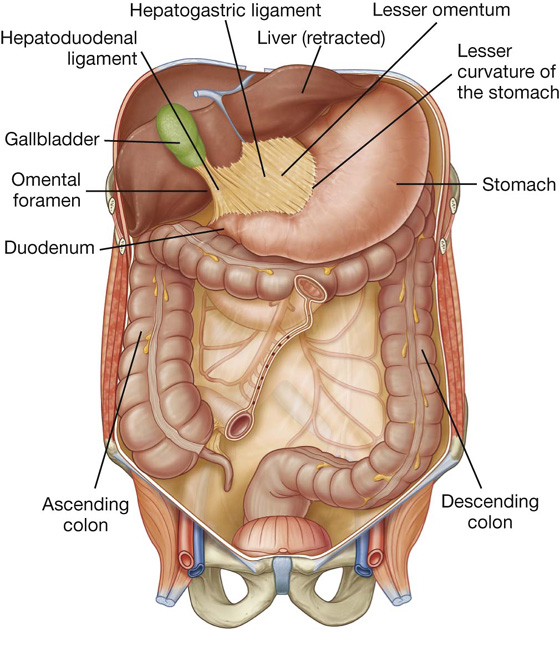
Fig. 4.37 Lesser omentum.
A thin membrane continuous with the peritoneal coverings of the anterior and posterior surfaces of the stomach and the first part of the duodenum, the lesser omentum is divided into:
 a medial hepatogastric ligament, which passes between the stomach and liver, and
a medial hepatogastric ligament, which passes between the stomach and liver, and
 a lateral hepatoduodenal ligament, which passes between the duodenum and liver.
a lateral hepatoduodenal ligament, which passes between the duodenum and liver.
The hepatoduodenal ligament ends laterally as a free margin and serves as the anterior border of the omental foramen (see Fig. 4.35). Enclosed in this free edge are the hepatic artery proper, the bile duct, and the portal vein. Additionally, the right and left gastric vessels are between the layers of the lesser omentum near the lesser curvature of the stomach.
Clinical app
The greater omentum
When a laparotomy is performed and the peritoneal cavity is opened, the first structure usually encountered is the greater omentum. This fatty double-layered vascular membrane hangs like an apron from the greater curvature of the stomach, drapes over the transverse colon, and lies freely suspended within the abdominal cavity. It is often referred to as the “policeman of the abdomen” because of its apparent ability to migrate to any inflamed area and wrap itself around the organ to wall off inflammation.
The greater omentum is also an important site for metastatic tumor spread. Direct omental spread by a transcoelomic route is common for carcinoma of the ovary.
Mesenteries
Mesenteries are peritoneal folds that attach viscera to the posterior abdominal wall. They allow some movement and provide a conduit for vessels, nerves, and lymphatics to reach the viscera and include:
 the mesentery—associated with parts of the small intestine,
the mesentery—associated with parts of the small intestine,
 the transverse mesocolon—associated with the transverse colon, and
the transverse mesocolon—associated with the transverse colon, and
 the sigmoid mesocolon—associated with the sigmoid colon.
the sigmoid mesocolon—associated with the sigmoid colon.
All of these are derivatives of the dorsal mesentery.
The mesentery is a large, fan-shaped, double-layered fold of peritoneum that connects the jejunum and ileum to the posterior abdominal wall (Fig. 4.38). Its superior attachment is at the duodenojejunal junction, just to the left of the upper lumbar part of the vertebral column. It passes obliquely downward and to the right, ending at the ileocecal junction near the upper border of the right sacro-iliac joint. In the fat between the two peritoneal layers of the mesentery are the arteries, veins, nerves, and lymphatics that supply the jejunum and ileum.
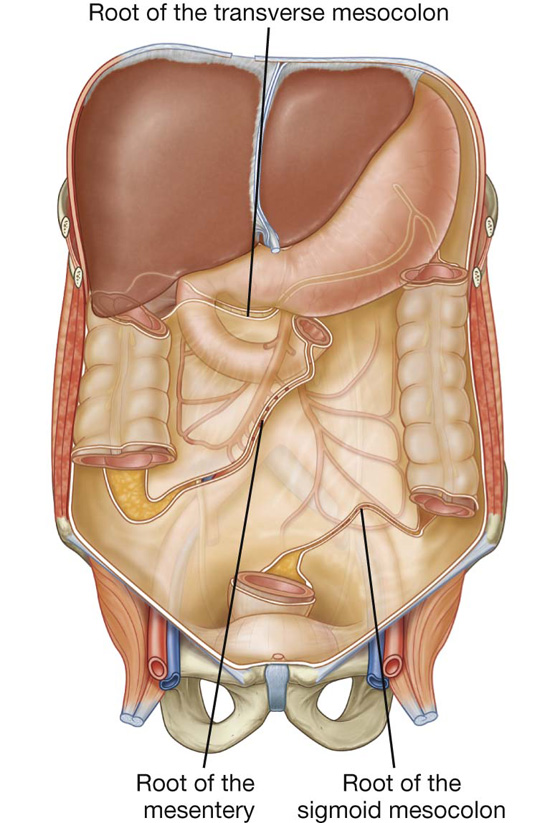
Fig. 4.38 Peritoneal reflections, forming mesenteries, outlined on the posterior abdominal wall.
The transverse mesocolon is a fold of peritoneum that connects the transverse colon to the posterior abdominal wall (Fig. 4.38, also see Fig. 4.34). Its two layers of peritoneum leave the posterior abdominal wall across the anterior surface of the head and body of the pancreas and pass outward to surround the transverse colon. Between its layers are the arteries, veins, nerves, and lymphatics related to the transverse colon. The anterior layer of the transverse mesocolon is adherent to the posterior layer of the greater omentum.
The sigmoid mesocolon is an inverted, V-shaped peritoneal fold that attaches the sigmoid colon to the abdominal wall (Fig. 4.38). The apex of the V is near the division of the left common iliac artery into its internal and external branches, with the left limb of the descending V along the medial border of the left psoas major muscle and the right limb descending into the pelvis to end at the level of vertebra SIII. The sigmoid and superior rectal vessels, along with the nerves and lymphatics associated with the sigmoid colon, pass through this peritoneal fold.
Ligaments
Peritoneal ligaments consist of two layers of peritoneum that connect two organs to each other or attach an organ to the body wall, and may form part of an omentum. They are usually named after the structures being connected. For example, the splenorenal ligament connects the left kidney to the spleen and the gastrophrenic ligament connects the stomach to the diaphragm.
Organs
Abdominal esophagus
The abdominal esophagus represents the short distal part of the esophagus located in the abdominal cavity. Emerging through the right crus of the diaphragm, usually at the level of vertebra TX, it passes from the esophageal hiatus to the cardial orifice of the stomach just left of the midline (Fig. 4.39).
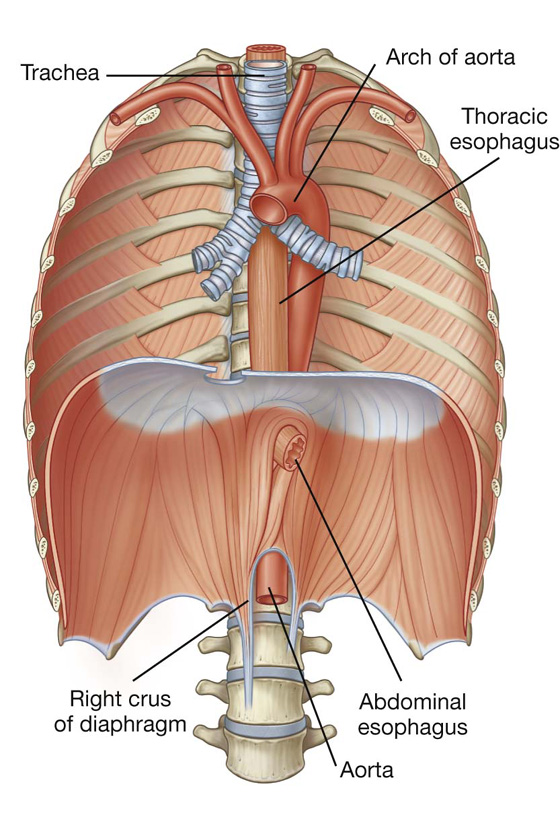
Fig. 4.39 Abdominal esophagus.
Associated with the esophagus, as it enters the abdominal cavity, are the anterior and posterior vagal trunks:
 The anterior vagal trunk consists of several smaller trunks whose fibers mostly come from the left vagus nerve; rotation of the gut during development moves these trunks to the anterior surface of the esophagus;
The anterior vagal trunk consists of several smaller trunks whose fibers mostly come from the left vagus nerve; rotation of the gut during development moves these trunks to the anterior surface of the esophagus; Similarly, the posterior vagal trunk consists of a single trunk whose fibers mostly come from the right vagus nerve, and rotational changes during development move this trunk to the posterior surface of the esophagus.
Similarly, the posterior vagal trunk consists of a single trunk whose fibers mostly come from the right vagus nerve, and rotational changes during development move this trunk to the posterior surface of the esophagus.The arterial supply to the abdominal esophagus (Fig. 4.40) includes:
 esophageal branches from the left gastric artery (from the celiac trunk), and
esophageal branches from the left gastric artery (from the celiac trunk), and
 esophageal branches from the left inferior phrenic artery (from the abdominal aorta).
esophageal branches from the left inferior phrenic artery (from the abdominal aorta).
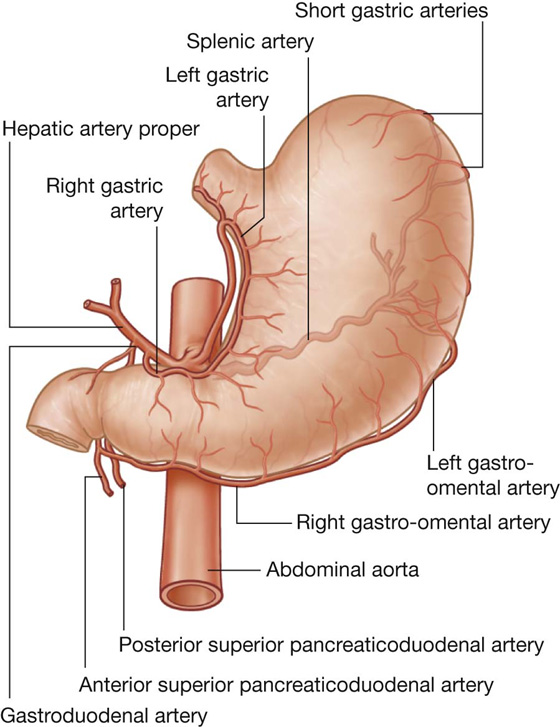
Fig. 4.40 Arterial supply to the abdominal esophagus and stomach.
Stomach
The stomach is the most dilated part of the gastrointestinal tract and has a J-like shape (Figs. 4.41, 4.42). Positioned between the abdominal esophagus and the small intestine, the stomach is in the epigastric, umbilical, and left hypochondrium regions of the abdomen.
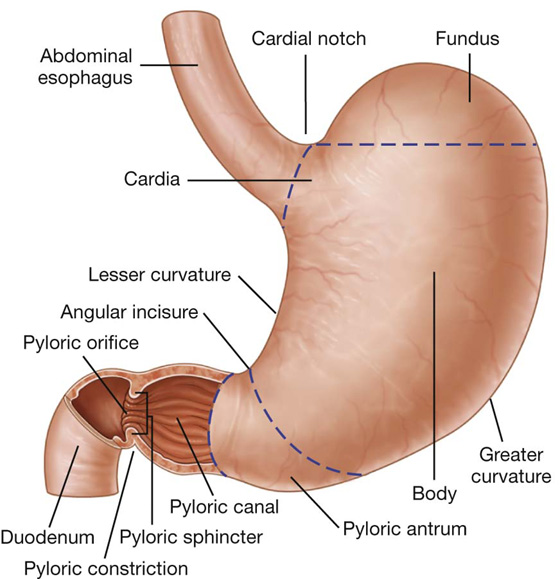
Fig. 4.41 Stomach.
Imaging app
Visualizing the stomach
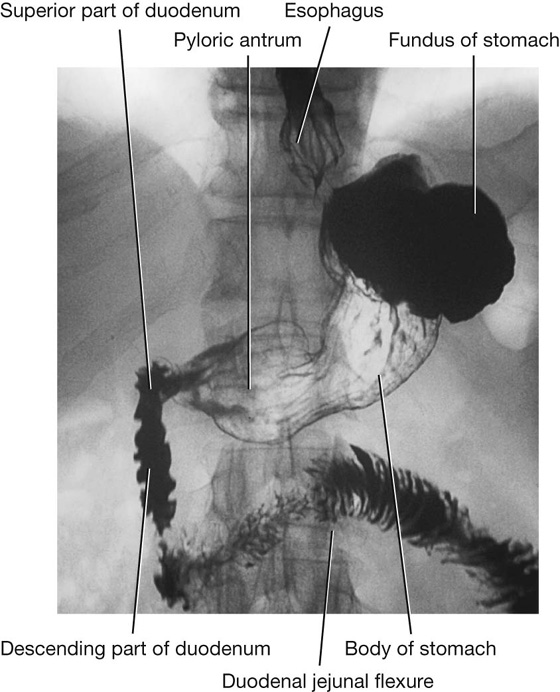
Fig. 4.42 Double contrast radiograph of the stomach and duodenum.
The stomach is divided into four regions (Fig. 4.41):
 the cardia, which surrounds the opening of the esophagus into the stomach;
the cardia, which surrounds the opening of the esophagus into the stomach;
 the fundus of stomach, which is the area above the level of the cardial orifice;
the fundus of stomach, which is the area above the level of the cardial orifice;
 the body of stomach, which is the largest region of the stomach; and
the body of stomach, which is the largest region of the stomach; and
 the pyloric part, which is divided into the pyloric antrum and pyloric canal and is the distal end of the stomach (Fig. 4.41).
the pyloric part, which is divided into the pyloric antrum and pyloric canal and is the distal end of the stomach (Fig. 4.41).
The most distal portion of the pyloric part of the stomach is the pylorus (Fig. 4.41). It is marked on the surface of the organ by the pyloric constriction and contains a thickened ring of gastric circular muscle, the pyloric sphincter, which surrounds the distal opening of the stomach, the pyloric orifice. The pyloric orifice is just to the right of midline in a plane that passes through the lower border of vertebra LI (the transpyloric plane).
Other features of the stomach include:
 the greater curvature, which is a point of attachment for the gastrosplenic ligament and the greater omentum;
the greater curvature, which is a point of attachment for the gastrosplenic ligament and the greater omentum; the lesser curvature, which is a point of attachment for the lesser omentum;
the lesser curvature, which is a point of attachment for the lesser omentum;
 the cardial notch, which is the superior angle created when the esophagus enters the stomach; and
the cardial notch, which is the superior angle created when the esophagus enters the stomach; and
 the angular incisure, which is a bend on the lesser curvature.
the angular incisure, which is a bend on the lesser curvature.
The arterial supply to the stomach (Fig. 4.40) includes:
 the left gastric artery from the celiac trunk,
the left gastric artery from the celiac trunk,
 the right gastric artery from the hepatic artery proper,
the right gastric artery from the hepatic artery proper,
 the right gastro-omental artery from the gastroduodenal artery,
the right gastro-omental artery from the gastroduodenal artery,
 the left gastro-omental artery from the splenic artery, and
the left gastro-omental artery from the splenic artery, and
 the posterior gastric artery from the splenic artery (variant and not always present).
the posterior gastric artery from the splenic artery (variant and not always present).
Small intestine
The small intestine is the longest part of the gastrointestinal tract and extends from the pyloric orifice of the stomach to the ileocecal fold. This hollow tube, which is approximately 6 to 7 m long with a narrowing diameter from beginning to end, consists of the duodenum, the jejunum, and the ileum.
Duodenum
The first part of the small intestine is the duodenum. This C-shaped structure, adjacent to the head of the pancreas, is 20 to 25 cm long and is above the level of the umbilicus; its lumen is the widest of the small intestine (Fig. 4.43). It is retroperitoneal except for its beginning, which is connected to the liver by the hepatoduodenal ligament, a part of the lesser omentum.
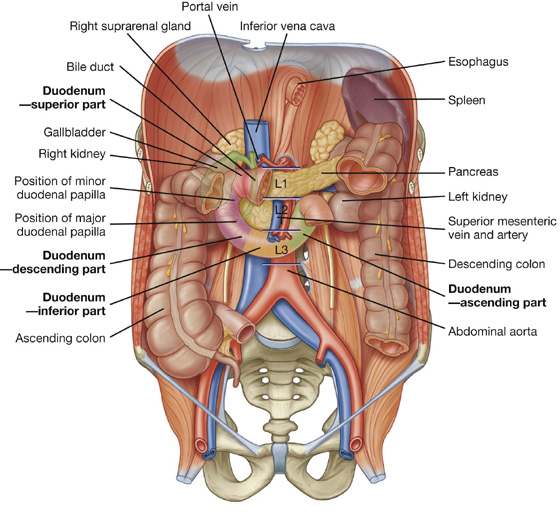
Fig. 4.43 Duodenum.
The duodenum is divided into four parts (Fig. 4.43).
 The superior part (first part) extends from the pyloric orifice of the stomach to the neck of the gallbladder, is just to the right of the body of vertebra LI, and passes anteriorly to the bile duct, gastroduodenal artery, portal vein, and inferior vena cava. Clinically, the beginning of this part of the duodenum is referred to as the ampulla or duodenal cap, and most duodenal ulcers occur in this part of the duodenum.
The superior part (first part) extends from the pyloric orifice of the stomach to the neck of the gallbladder, is just to the right of the body of vertebra LI, and passes anteriorly to the bile duct, gastroduodenal artery, portal vein, and inferior vena cava. Clinically, the beginning of this part of the duodenum is referred to as the ampulla or duodenal cap, and most duodenal ulcers occur in this part of the duodenum. The descending part (second part) of the duodenum is just to the right of midline and extends from the neck of the gallbladder to the lower border of vertebra LIII. Its anterior surface is crossed by the transverse colon, posterior to it is the right kidney, and medial to it is the head of the pancreas. This part of the duodenum contains the major duodenal papilla, which is the common entrance for the bile and pancreatic ducts, and the minor duodenal papilla, which is the entrance for the accessory pancreatic duct, and the junction of the foregut and the midgut just below the major duodenal papilla.
The descending part (second part) of the duodenum is just to the right of midline and extends from the neck of the gallbladder to the lower border of vertebra LIII. Its anterior surface is crossed by the transverse colon, posterior to it is the right kidney, and medial to it is the head of the pancreas. This part of the duodenum contains the major duodenal papilla, which is the common entrance for the bile and pancreatic ducts, and the minor duodenal papilla, which is the entrance for the accessory pancreatic duct, and the junction of the foregut and the midgut just below the major duodenal papilla. The inferior part (third part) of the duodenum is the longest section, crossing the inferior vena cava, the aorta, and the vertebral column (Figs. 4.42, 4.43). It is crossed anteriorly by the superior mesenteric artery and vein.
The inferior part (third part) of the duodenum is the longest section, crossing the inferior vena cava, the aorta, and the vertebral column (Figs. 4.42, 4.43). It is crossed anteriorly by the superior mesenteric artery and vein.
 The ascending part (fourth part) of the duodenum passes upward on, or to the left of, the aorta to approximately the upper border of vertebra LII and terminates at the duodenojejunal flexure.
The ascending part (fourth part) of the duodenum passes upward on, or to the left of, the aorta to approximately the upper border of vertebra LII and terminates at the duodenojejunal flexure.This duodenojejunal flexure is surrounded by a fold of peritoneum containing muscle fibers called the suspensory muscle (ligament) of duodenum (ligament of Treitz).
The arterial supply to the duodenum (Fig. 4.44) includes:
 branches from the gastroduodenal artery,
branches from the gastroduodenal artery,
 the supraduodenal artery from the gastroduodenal artery,
the supraduodenal artery from the gastroduodenal artery,
 duodenal branches from the anterior superior pancreaticoduodenal artery (from the gastroduodenal artery),
duodenal branches from the anterior superior pancreaticoduodenal artery (from the gastroduodenal artery), duodenal branches from the posterior superior pancreaticoduodenal artery (from the gastroduodenal artery),
duodenal branches from the posterior superior pancreaticoduodenal artery (from the gastroduodenal artery), duodenal branches from the anterior inferior pancreaticoduodenal artery (from the inferior pancreaticoduodenal artery—a branch of the superior mesenteric artery),
duodenal branches from the anterior inferior pancreaticoduodenal artery (from the inferior pancreaticoduodenal artery—a branch of the superior mesenteric artery), duodenal branches from the posterior inferior pancreaticoduodenal artery (from the inferior pancreaticoduodenal artery—a branch of the superior mesenteric artery), and
duodenal branches from the posterior inferior pancreaticoduodenal artery (from the inferior pancreaticoduodenal artery—a branch of the superior mesenteric artery), and the first jejunal branch from the superior mesenteric artery.
the first jejunal branch from the superior mesenteric artery.
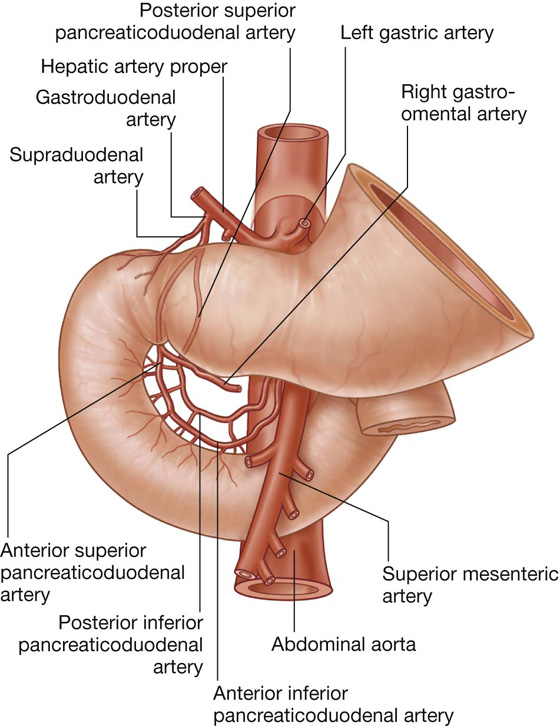
Fig. 4.44 Arterial supply to the duodenum.
Jejunum
The jejunum and ileum make up the last two sections of the small intestine (Fig. 4.45
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


