A Survey of Frozen Section Literature
Jie Song
The intraoperative consultation utilizing frozen section is employed by all practicing pathologists. However, the use of this technique in clinical management may be a parochial issue within a given institution. Details regarding utilization or potentially valuable practice tips among pathologists may not be regarded by journal editors with the same importance as gene research, the description of a new tumor variant or a new antibody for immunohistochemistry (IHC). Nonetheless, communication among pathologists on the issue of frozen section is potentially important for daily practice and patient care. It is the intent here to look at pathology literature related specifically to frozen section as an indicator of pathologists’ intercommunication on this vital subject.
PubMed searches using “frozen section” and “intraoperative” as keywords identified 901 English-language articles between January 1, 1980, and July 1, 2012. Only articles pertaining to anatomic pathology diagnosis were included. There has been a steady increase in the number of publications each year, particularly after the year 2000 (Fig. 2.1). The vast majority of these articles have focused on a single organ system. The top five ranked by the number of publications are breast (132), thyroid (94), ovary (74), uterus (68), and skin (50). The gynecologic system ranks at the top among all systems, with 151 articles published in this period of time (Table 2.1).
Publications have increased for essentially all organ systems, particularly over the last decade (Fig. 2.2). Breast and the gynecologic system have undergone the most dramatic growth, while nervous system and bone/soft tissue have remained relatively stable. The publication increase, especially in those areas which have shown rapid evolvement of frozen section use, may reflect specific changes in clinical practice in a particular venue as well as increases of academic interest and clinical research.
Further analysis of the numbers in Figure 2.2 has indeed shown periodic changes in the main topic of these articles, even for the same organ. The paradigm shifts in clinical practice, driven by evolving demand of surgical oncology and new technology, are best illustrated by the breast category, comprising the largest number of publications for a single organ. Articles before the year 2000 mainly focused on making a primary diagnosis on
frozen sections of incisional or excisional breast biopsies (see Chapter 8). This was a common practice at a time when breast tumors tended to be large and palpable when discovered. A diagnosis of malignancy by frozen section led to a mastectomy, thus achieving diagnosis and definite surgical therapy in a single procedure. This practice has gradually fallen out of favor with the rise of mammogram screening, stereotactic- or ultrasound-guided
needle core biopsies and the availability of breast conservation surgery. Frozen section diagnosis is not as accurate on these small, nonpalpable lesions discovered by screening (1). Perhaps more importantly, the demand for frozen section as a primary diagnostic tool no longer exists, since immediate excision or mastectomy after needle core biopsy is neither beneficial nor desired. Although occasional studies published in the 1990s advocated frozen section diagnosis on needle core biopsies (2), the common current practice for these biopsies is to be interpreted on routine paraffin-embedded permanent sections, essentially eliminating frozen section as a primary diagnostic method (3,4,5).
frozen sections of incisional or excisional breast biopsies (see Chapter 8). This was a common practice at a time when breast tumors tended to be large and palpable when discovered. A diagnosis of malignancy by frozen section led to a mastectomy, thus achieving diagnosis and definite surgical therapy in a single procedure. This practice has gradually fallen out of favor with the rise of mammogram screening, stereotactic- or ultrasound-guided
needle core biopsies and the availability of breast conservation surgery. Frozen section diagnosis is not as accurate on these small, nonpalpable lesions discovered by screening (1). Perhaps more importantly, the demand for frozen section as a primary diagnostic tool no longer exists, since immediate excision or mastectomy after needle core biopsy is neither beneficial nor desired. Although occasional studies published in the 1990s advocated frozen section diagnosis on needle core biopsies (2), the common current practice for these biopsies is to be interpreted on routine paraffin-embedded permanent sections, essentially eliminating frozen section as a primary diagnostic method (3,4,5).
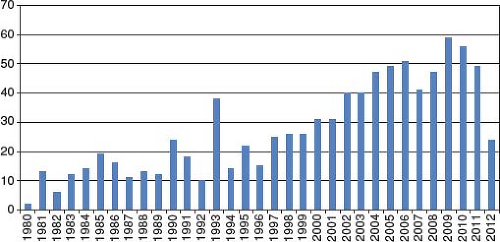 Figure 2.1 The number of PubMed-indexed journal articles pertaining to frozen section diagnosis from 1980 to 2012. (Note: 2012 data is based on the first 6 months only.) |
Table 2.1 The Number of Journal Articles from 1980 to 2012 by Organ System | ||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||
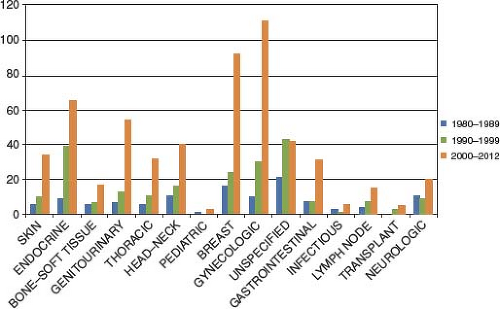 Figure 2.2 The number of journal articles by organ system broken down by decade. “Unspecified” are articles that discuss frozen section in general, such as technology, history, and diagnostic accuracy, without being limited to a certain organ system. “Lymph node” group designates articles about lymph node evaluation without specifying any organ system as the source of primary disease. (Note: 2012 data is based on the first 6 months only.) |
At the same time, more and more articles appeared discussing frozen section for margin evaluation and sentinel lymph node (SLN) evaluation in breast cancer, in order to facilitate new conservative surgical techniques. Lymph nodes, particularly SLNs, now account for the majority of articles about breast cancer frozen section. This trend is clearly demonstrated on a bar graph (Fig. 2.3). It is interesting to point out that, even after 2000, a small number of articles continued to discuss frozen section of breast lesions for primary diagnostic purpose. However, none of these articles originates from US institutions, reflecting the variations in medical practice across the world.
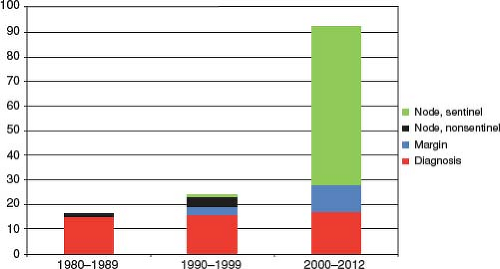 Figure 2.3 The number of journal articles about breast cancer frozen section, divided by main topics: Primary diagnosis, margin evaluation, and lymph node assessment. (Note: 2012 data is based on the first 6 months only.) |
Telepathology and Frozen Section
Over 30 articles have been published discussing telepathology in the setting of frozen section. The majority of these articles appeared over the past 10 years. Telepathology is the delivery of anatomic pathology diagnosis at a distance, through digital images transmitted over a network, which allows the physical separation of a pathologist from the glass slides (6). Compared to regular anatomic pathology service, frozen section is more time sensitive, and may involve a solo pathologist who may not have access to a colleague’s consultation opinion due to time and distance constraints. Additional variations may include large medical centers in which the frozen section area is distant from the main pathology offices, some rural or small hospitals and surgical centers that may not have on-site pathologists for full-time frozen section coverage. These factors have made telepathology a particularly attractive option for frozen section service. The technical requirements of telepathology for frozen section include fast image acquisition, reliable network transmission, and smooth digital image viewing in order for the remote pathologist to render accurate diagnosis in a timely manner. The additional time cost, compared to conventional frozen section, has to be limited to the range of a few minutes, in order for telepathology to become a feasible approach.
Telepathology for frozen section was first published in 1991 (7). This pioneer system was based on a motorized microscope with a mounted video camera that was remotely controlled by a pathologist located in an office 420 km away. Regular streaming video was also used simultaneously for the pathologist to guide the on-site surgeon on gross examination and sampling of specimen. Mixed live (256 × 286 pixels) and still (576 × 720 pixels)
microscopic images were transmitted to achieve a balance between speed and quality. This system was successfully used in 17 frozen section diagnoses (7). Since then, a variety of telepathology systems have been developed for frozen section service, and the vast majority of them can be classified into three types (Fig. 2.4



microscopic images were transmitted to achieve a balance between speed and quality. This system was successfully used in 17 frozen section diagnoses (7). Since then, a variety of telepathology systems have been developed for frozen section service, and the vast majority of them can be classified into three types (Fig. 2.4
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
