84 CASE 84
A 32-year-old woman has an appointment with her gynecologist for a normal prenatal checkup.
PATHOPHYSIOLOGY OF KEY SYMPTOMS
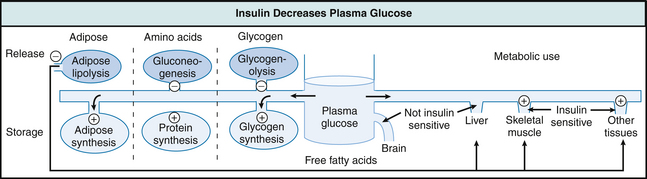
Insulin is produced by the pancreas in response to an elevation in blood glucose. Insulin acts to decrease plasma glucose by stimulating cellular glucose uptake in a variety of tissues, especially the liver and skeletal muscle (Fig. 84-1). One consequence of the changing endocrine environment is that the maternal tissues lose their sensitivity to insulin. As tissues become less responsive to glucose, fasting plasma glucose levels rise, plasma insulin levels rise, and the body is unable to efficiently store ingested glucose. Gestational diabetes results from a loss of tissue insulin sensitivity during the third trimester of pregnancy and resembles type 2 diabetes mellitus. Gestational diabetes develops in around 4% of pregnancies in the United States.
< div class='tao-gold-member'>
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


