70 CASE 70
A 38-year-old man is transported to the emergency department after having fainted at home.
PATHOPHYSIOLOGY OF KEY SYMPTOMS
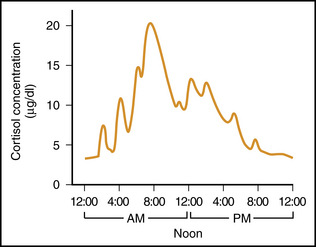
Cortisol exhibits a marked diurnal variation in plasma levels, with the highest level at 8 AM being more than four times as high as the lowest level at night (Fig. 70-1). Consequently, a patient’s plasma cortisol level must be matched against an appropriate range for that time of day.
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


