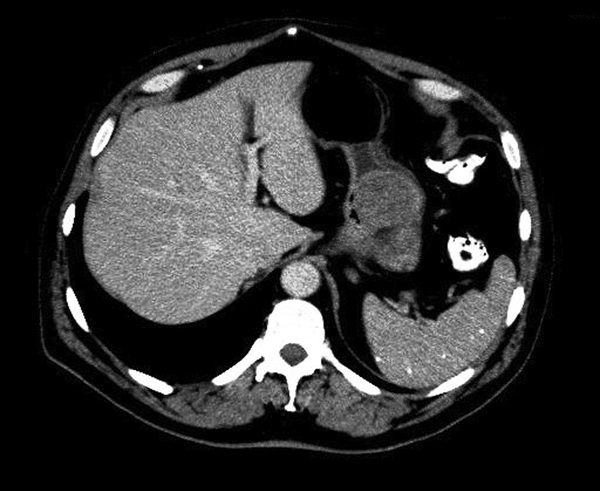
Monisha Bhanote, Daniel Martinez In the absence of a malabsorptive pathology or extreme malnutrition, iron deficiency anemia is generally caused by chronic blood loss of some time. It is typical for the source of bleeding to be from a gastrointestinal source. Referring this patient for a colonoscopy because of his symptoms of bright red blood per rectum in the setting of iron deficiency anemia was the correct decision at the time. However, the presence of one source of bleeding does not itself rule out the possibility of other sources of bleeding. Generally speaking, patients with an iron deficiency anemia should receive both a colonoscopy and an upper endoscopy to rule out other sources of bleeding such as a gastric or duodenal ulcer. This is especially the case when the patient is still iron dependent after his polyps are removed and his hemorrhoids are treated with a high-fiber diet. When the source of bleeding has been removed, a patient’s iron stores should replenish in a few months of oral iron supplementation. Failure to do so should have prompted the PMD to evaluate further sources of occult bleeding. The differential diagnosis for new-onset abdominal pain is very wide, and a good way to think about common causes is by considering the potential organs involved. In the left upper quadrant, the pancreas can be involved by pancreatitis and the stomach can be involved by a peptic ulcer or a mass. In the right upper quadrant, the hepatobiliary system can be involved by cholecystitis, cholangitis, or biliary colic. In the left lower and right lower quadrants, the small intestines and colon can be involved with diverticulitis, appendicitis, bowel obstruction, inflammatory bowel disease, and colonic masses. The possibility of bony metastasis or metastasis to other organs should be considered in a patient with a previously diagnosed malignancy. Another rare consideration is aortic dissection or ruptured aneurysm in the right clinical setting. If any of these are reasonable suspicions based on his clinical presentation, it is appropriate to order a computed tomography (CT) scan of the abdomen/pelvis with intravenous (IV) contrast. (The addition of oral [PO] contrast can also help evaluate the bowel better for a small bowel obstruction.) Given the patient’s tachycardia and new and acute epigastric pain, basic labs and a CT scan of the abdomen and pelvis with IV and PO contrast is ordered. White blood cell (WBC) count is 8000 cells/µL, hemoglobin is 14 g/dL, and mean corpuscular volume (MCV) is 82 fL/cell. The patient’s CT scan is done quickly, and the radiologist evaluates the results. A 3.6-cm submucosal mass is found in the stomach (see Fig. 56.1). There is no evidence of pancreatitis, cholecystitis, appendicitis, or small bowel obstruction. He does have sigmoid diverticulosis, but there is no evidence of diverticulitis. No lymphadenopathy is appreciated. Submucosal masses can be benign or malignant, and the differential diagnosis of a submucosal mass can be divided into mesenchymal versus nonmesenchymal lesions (see Table 56.1). The CT scan shows no evidence of active bleeding or infection, and his vital signs improve with moderate pain control. The patient is therefore discharged with follow-up with his gastroenterologist for an upper endoscopy and possible endoscopic ultrasound–guided fine needle aspiration (EUS-FNA). During the upper endoscopy, the stomach shows a protruding mass with intact overlying mucosa (see Fig. 56.2
A 70-Year-Old Male With Iron Deficiency Anemia
Does the patient still need iron supplementation?
What are some considerations of abdominal pain in this patient?
What is the differential diagnosis of a gastric submucosal mass?
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


56 A 70-Year-Old Male With Iron Deficiency Anemia
Case 56
{kind=link}
