52 CASE 52
LABORATORY STUDIES
Barium esophagography: Esophageal dilation, a loss of esophageal peristalsis, poor esophageal emptying, and a smooth symmetrical “bird’s beak” tapering of the distal esophagus.
PATHOPHYSIOLOGY OF KEY SYMPTOMS
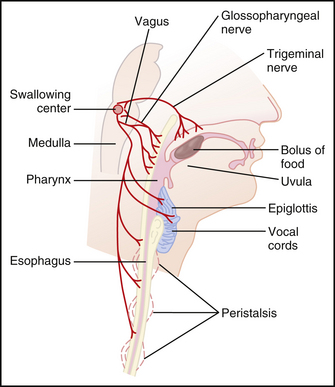
The swallowing reflex begins as a voluntary action in the mouth and continues as an involuntary reflex through the pharynx and the esophagus (Fig. 52-1). Esophageal peristalsis results from two muscular actions: a contraction of the muscle proximal to the bolus of food and a relaxation of the muscle distal to the bolus of food. As the wave of relaxation progresses down the esophagus, the bolus of food is moved down the esophagus by the wave of contraction proximal to the bolus.
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


