49 CASE 49
PATHOPHYSIOLOGY OF KEY SYMPTOMS
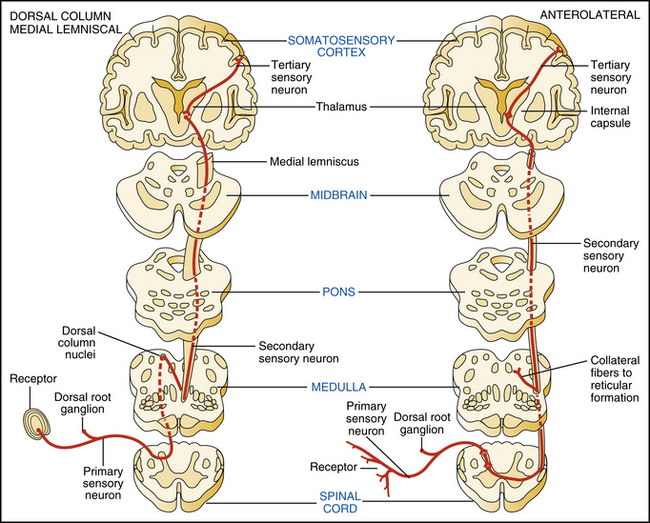
Spinal cord sensory transmission ascends predominantly in the dorsal columns and the anterolateral tracts. Sensory nerves that transmit the modalities of fine touch, vibration, and proprioception enter the spinal cord at the dorsal root and ascend ipsilaterally to the medulla. A second-order sensory neuron crosses the midline forming the medial lemniscus and carries the information to the thalamus. The tertiary sensory neuron ascends from the thalamus to the somatosensory cortex. In contrast, pain and temperature sensory inputs travel through the anterolateral pathway. Sensory neurons enter the dorsal root and synapse in the dorsal horn of the gray matter of the ipsilateral cord. Second-order neurons send their axons across the midline to the contralateral anterolateral tract in which they ascend to make synaptic connection in the thalamus. The third neuron in the pathway projects to the somatosensory cortex. The anterolateral system is highly divergent; and as the pathway ascends, collaterals relay information to many targets, including the reticular formation and periaqueductal gray matter of the brain stem. Within the spinal cord, somatotopic organization is maintained, because nerve fibers originating from the upper parts of the body are carried in the more medial portions of the tract and nerve fibers originating from the lower parts of the body are carried in the more lateral portions of the tract (Fig. 49-1).
< div class='tao-gold-member'>
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


