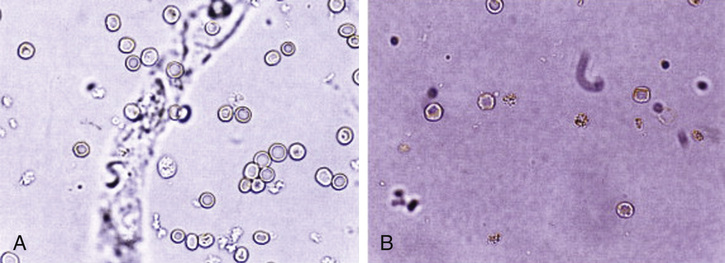
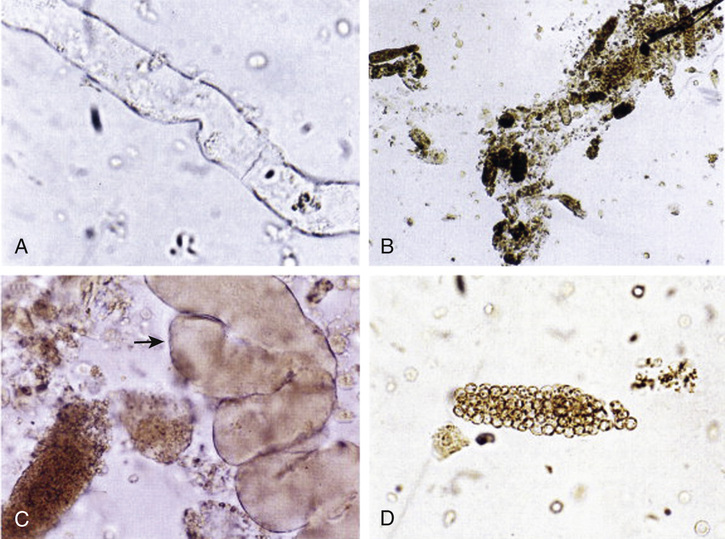
Ravi Lakdawala, Joseph Abdelmalek When evaluating dark-colored urine, you must determine whether the etiology is blood or pigment. True hematuria signifies the presence of red blood cells and can be classified as either gross (i.e., visible to the eye) or microscopic (which requires microscopy for diagnosis). Once the presence of red blood cells is confirmed, the source of hematuria can be characterized as coming from within the kidney (intrarenal, or upper urinary tract bleeding) or from outside the kidney (extrarenal, or lower urinary tract). Intrarenal sources of bleeding include glomerulonephritis, vasculitis, pyelonephritis, and malignancy. Causes of extrarenal bleeding include nephrolithiasis, bladder or urethral infections, malignancy, or trauma. About 95% of patients with hypertension have primary or essential hypertension, where blood pressure is greater than 140/90 mm Hg with no specific identifiable etiology. The likely pathogenesis for elevated blood pressure in these individuals is multifactorial, including genetics, congenital renal impairment, and renal injury leading to impaired sodium excretion with subsequent volume expansion and elevated blood pressure. Secondary hypertension can be due to renal parenchymal or glomerular diseases, renovascular disease, endocrine diseases such as Cushing syndrome and aldosteronism; preeclampsia or eclampsia, as well as obstructive sleep apnea and drug-induced causes due to sympathomimetics, glucocorticoids, nonsteroidal antiinflammatory drugs (NSAIDs), and oral contraceptives. Risk factors for a secondary cause of hypertension include the sudden onset of hypertension, very young or very old age at onset of hypertension, and resistant hypertension. Resistant hypertension is defined by the inability to control blood pressure while on at least three antihypertensive medications at the maximum tolerated dose. In this case, the presence of hypertension in a 22-year-old without a family history suggests a secondary cause. Laboratory testing reveals a normal complete blood count, electrolytes, creatinine, and liver function. His urine dipstick is positive for 3+ blood and 2+ protein but negative for leukocyte esterase, nitrites, ketones, bilirubin, and glucose. Microscopic analysis of the urine shows >50 red blood cells per high power field, dysmorphic red blood cells (Fig. 39.1), 6 to 10 red blood cell casts per high power field (Fig. 39.2), and 0 to 3 white blood cells per high power field, with no crystals or bacteria.
A 22-Year-Old Male With Hematuria
What is the significance of dark-colored urine?
What is the significance of this patient’s hypertension?
39 A 22-Year-Old Male With Hematuria
Case 39