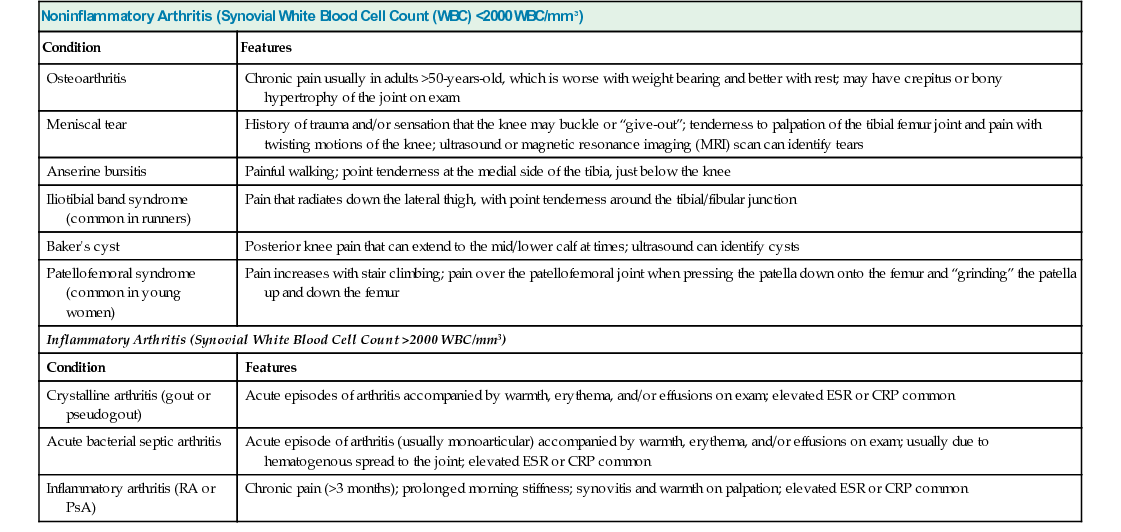
R. Michelle Koolaee Table 36.1 summarizes some common causes of knee pain. There are several key questions to always ask anyone who presents to you with knee pain: This is a 68-year-old overweight male with no history of trauma who presents with chronic right knee pain that is worse with weight-bearing activity, medial joint space tenderness with a small effusion, and noninflammatory synovial fluid. Synovial fluid aspiration is a critical part of narrowing down the differential diagnosis for anyone with joint pain. Noninflammatory fluid, as in this case, is characterized by a synovial fluid WBC count of less than 2000 WBC/mm3. A WBC count of 750 WBC/mm3 essentially rules out any type of inflammatory arthritis; this includes crystalline arthritis, RA, PsA, or septic arthritis, to name a few. Even if synovial fluid analysis were not available, the chronicity of the patient’s knee pain would make crystalline or acute bacterial septic arthritis unlikely. As mentioned earlier, the short duration of morning stiffness would make RA or PsA unlikely. Table 36.1 lists common causes of knee pain with noninflammatory fluid. The clinical presentation here is most consistent with OA, although it is important to also be aware of other conditions that can often be present concurrently in someone with a history of OA. The lack of a history of trauma or sensation that the knee is going to “give out” or buckle makes the possibility of an acute meniscal or ligament tear very unlikely. The medial location of the knee pain makes iliotibial band syndrome or a baker’s cyst unlikely as well. A negative patellofemoral grind test makes patellofemoral syndrome unlikely. Anserine bursitis is a cause of focal tenderness at the medial tibial plateau, just below the knee; however, this patient’s pain is at the medial joint space.
A 68-Year-Old Male With Right Knee Pain
How does the history help to narrow your differential diagnosis?
What is your differential diagnosis?
What is the pathogenesis of OA?
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


36 A 68-Year-Old Male With Right Knee Pain
Case 36