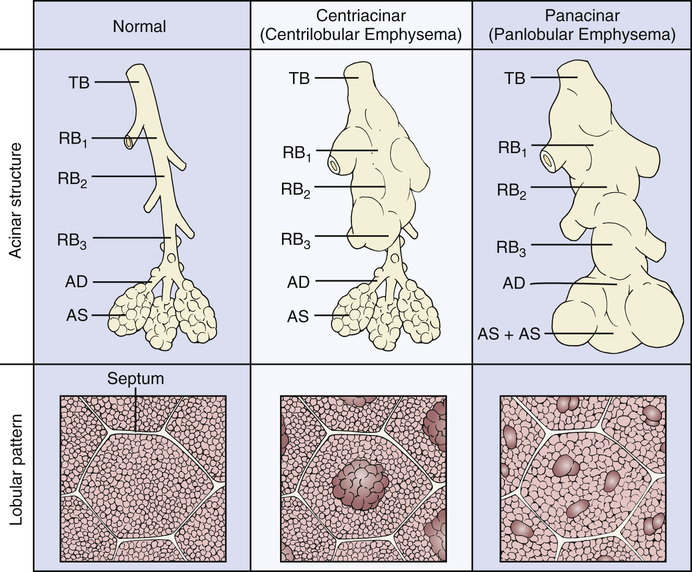
Andrew Morado, Raj Dasgupta, Ahmet Baydur Anytime shortness of breath or dyspnea are encountered, it is best to keep the differential broad to help organize a diagnostic approach. The three main categories are the lungs, heart, and anemia. In an older male such as this, the most likely causes are cardiac or pulmonary in nature, though you can never exclude less common causes on history alone. There is no immediate history of coronary artery disease, chest pain, or orthopnea that might suggest congestive heart failure (CHF) as a potential etiology. Additionally, a productive cough could support a primary pulmonary pathology as a cause of his symptoms, though CHF and other cardiac etiologies such as arrhythmias and a dilated left atrium can be other potential culprits. Anemia, regardless of the cause, can manifest as dyspnea on exertion because of decreased oxygen delivery to tissues. Heart failure can be due to a low ejection fraction (systolic dysfunction), most commonly caused by myocardial infarction, or with preserved ejection fraction (diastolic dysfunction), which is strongly associated with long-standing, poorly controlled hypertension. Regardless of the type, the common complaints typically are dyspnea with exertion, orthopnea reported as need to remain upright while sleeping, and peripheral edema. With the absence of orthopnea and lower extremity edema, CHF becomes lower on the differential while pulmonary causes remain high. On exam, he is a thin male in no distress. The temperature is 37.9 °C (100.3 °F), blood pressure is 118/70 mm Hg, pulse rate is 110/min, respiration rate is 28/min, and oxygen saturation is 86% on room air. Heart sounds are distant. He exhibits an increased anterior/posterior diameter of his chest wall. Breath sounds are faint with end expiratory wheezes diffusely. There is no clubbing or lower extremity edema present. His faint heart and breath sounds suggest increased lung volumes, as does his chest wall diameter (barrel chest; see Fig. 15.1). His small stature is typical of patients with COPD while the absence of peripheral edema further refutes CHF. Clubbing is almost never seen with emphysema or chronic bronchitis (unlike in cystic fibrosis, bronchiectasis, or congenital heart disease). This is a 66-year-old male with progressive dyspnea on exertion, productive cough, and a 60 pack-year smoking history. Physical exam demonstrates evidence of hyperinflation and obstructive airway disease. COPD remains number one on the differential. We gave consideration earlier to left heart failure as it can cause dyspnea as well as wheezing if significant pulmonary edema is present. However, the absence of other classic history and exam findings such as elevated jugular venous pressure (JVP), S3 gallop, or orthopnea makes it less likely. Other considerations are other causes of obstructive airway disease. Chronic asthmatics could present in such a way, though he denies having a history of asthma as a younger male or child. He is too old to be newly diagnosed with cystic fibrosis. Alpha-1 antitrypsin (A1AT) deficiency is a definite consideration but is still less likely than COPD as a cause of this patient’s symptoms. (A1AT deficiency typically presents at a young age, especially if patients are homozygous for the mutation. Other clues to the diagnosis are necrotizing panniculitis, a rare skin lesion, and abnormalities in liver enzymes.) Step 1 Basic Science Pearl Emphysema or destruction of lung parenchyma can have varying patterns depending on the etiology of disease. For example, A1AT tends to present with panacinar emphysema, whereas smoking typically causes centrilobular emphysema. The difference pathologically is how the secondary pulmonary lobule is affected. In Figure 15.2, the functional unit of the lung otherwise known as the secondary pulmonary lobule is shown and typically houses 3 to 12 acini. Centrilobular emphysema involves loss of the proximal respiratory bronchiole within the acinus but sparing of distal alveolitis. This sparing of lung parenchyma produces the effect of normal- and abnormal-appearing lung that can be discerned by the naked eye and typically involves the upper lobes. In contrast, panacinar emphysema results in destruction of the entire acinus and mainly affects the lower lobes. Basic labs including a complete blood count (CBC) and basic metabolic panel (BMP) should be ordered, as they can reveal erythrocytosis suggesting chronic hypoxemia, though anemia is the most common blood abnormality, while an elevated bicarbonate suggests carbon dioxide retention. A1AT enzyme levels should be ordered to rule out this diagnosis.
A 66-Year-Old Male With Progressive Dyspnea on Exertion
With shortness of breath, what organ systems should be considered as a potential cause?
What clues in the history might point toward CHF?
What is your differential diagnosis?
What labs would you order and why?
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


15 A 66-Year-Old Male With Progressive Dyspnea on Exertion
Case 15