CHAPTER 50 Wrist and hand
SKIN AND SOFT TISSUE
SKIN
Skin creases and fingerprints
Flexure lines commonly crease the skin across the flexor surfaces of the wrist and hand (Fig. 50.1). Though not all directly over their functionally related subjacent skeletal joints, they are produced by adhesion of the skin to subjacent deep fascia and are sites of folding of the skin during movement. These flexures are useful landmarks. Less regular, but quite prominent, crease-line complexes are centred over the dorsal (extensor) aspects of the radiocarpal, carpal, metacarpophalangeal and interphalangeal joints. They are mainly transverse but display varying curvatures. During flexion the dorsal skin is stretched and the lines become less prominent (but can still be identified). During extension the now redundant skin becomes increasingly puckered and the lines are finally maximally prominent. (For a general review of ‘skin lines’ see p. 160.)
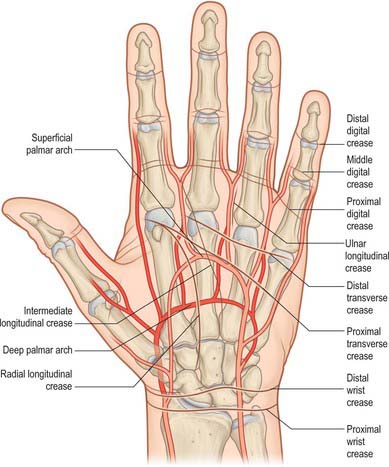
Fig. 50.1 Relation of the skin flexure lines and palmar arterial arches to the bones of the left hand.
(Adapted from Drake, Vogl and Mitchell 2005.)
The second to fifth digits show proximal, middle and distal sets of transverse lines. The proximal, often double, are at the digital roots, approximately 2 cm distal to the metacarpophalangeal joints. The middle lines are typically double, the proximal line lying directly over the proximal interphalangeal joint. The distal lines are usually single, and lie proximal to the distal interphalangeal joints: their levels are sometimes marked by a fainter, more distal line. The free pollicial base is partly encircled by a line which starts on the radial side and crosses distally over the metacarpophalangeal joint to end between the thumb and index finger level with the base of the proximal pollicial phalanx. There is a second, shorter crease usually 1 cm distal to this line. There are two lines comparable to the middle digital lines in other digits opposite the interphalangeal joint of the thumb (see also p. 160).
Cutaneous vascular supply
The skin of the volar aspect of the wrist is supplied directly by cutaneous branches from the superficial palmar branch of the radial artery, the ulnar artery and occasionally the median artery if it is large enough (Fig. 50.2). The skin over the thenar eminence is supplied by small perforating branches from the superficial palmar branch of the radial artery and the princeps pollicis. The skin over the hypothenar eminence is supplied by perforating branches from the ulnar artery, some of which pass through palmaris brevis. The remainder of the palm is supplied by small perforating branches from the common palmar digital arteries which pierce the palmar aponeurosis, and small branches from the radialis indicis artery. The blood supply to the volar aspect of the digital skin comes from small branches from each digital artery. At the level of the distal phalanx the two digital arteries typically form an H-shaped anastomosis from which cutaneous perforators fan out within the pulp. Deep digital veins accompanying the digital arteries are usually very small and frequently absent. More commonly, superficial palmar veins tend to pass dorsally and drain into the larger superficial dorsal venous system.
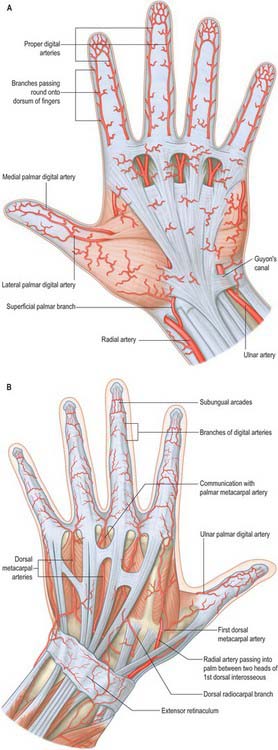
The blood supply to the dorsum of the fingers comes proximally from the terminal branches of the dorsal metacarpal arteries – supplying a region as far distally as the proximal interphalangeal joint – as well as from dorsal branches of the palmar digital arteries which are given off at each phalangeal level. At the level of the distal phalanx the cutaneous supply comes from three dorsal arcades: a superficial arcade over the base of the distal phalanx, and two distal subungual arcades. The skin of the dorsum of the thumb is supplied by longitudinal axial branches of the princeps pollicis and dorsal branches from the palmar digital arteries.
Cutaneous innervation
The skin of the volar aspect of the wrist is innervated by the terminal branches of the lateral and medial cutaneous nerves of the forearm. The skin of the palm is innervated by the palmar branches of the ulnar nerve and the palmar branch of the median nerve (Fig. 50.3; see also Fig. 50.45. The skin of the volar aspect of the thumb, index, middle and radial aspect of the ring fingers is supplied by cutaneous branches of the median nerve, while that of the little finger and ulnar side of the ring finger is supplied by the ulnar nerve.


NAIL APPARATUS
The nail apparatus consists of the nail plate, proximal and lateral nail folds, nail matrix, nail bed and hyponychium. It is described on page 154.
SOFT TISSUE
Palmar fascial complex
The palmar fascia is a three-dimensional ligamentous system composed of longitudinal, transverse and vertical fibres (Fig. 50.4).
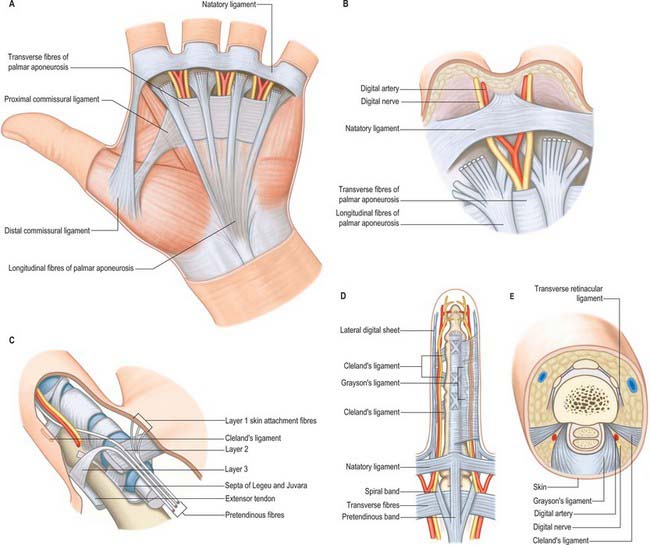
Longitudinal fibre system
The longitudinal fibres represent the phylogenetically degenerated metacarpophalangeal joint flexor. They run distally from the palmaris longus tendon or the flexor retinaculum of the wrist across the whole width of the central third of the palm, producing four well-defined longitudinal bundles to the index, middle, ring and little fingers. A less well-defined bundle passes to the thumb. Distal to the transverse fibres of the palmar aponeurosis the longitudinal fibres pass in three layers (McGrouther 1982). The most superficial longitudinal fibres (layer 1) are inserted superficially into the skin of the distal palm between the distal palmar crease and the proximal digital crease. Some superficial fibres pass distally into the palmar midline of the digit. Deeper longitudinal fibres (layer 2) pass deep to the natatory ligament and neurovascular bundles into the apex of the web space skin and into the fingers themselves where they are continuous with Cleland’s ligaments and the lateral digital sheet. These are known as the spiral bands of Gosset. Deeper still, the longitudinal fibres in layer 3 perforate the deep transverse metacarpal ligament to pass around the sides of the metacarpophalangeal joint and attach to the metacarpal bone and proximal phalanx, and extensor tendon.
Transverse fibre system
Digital fascial complex
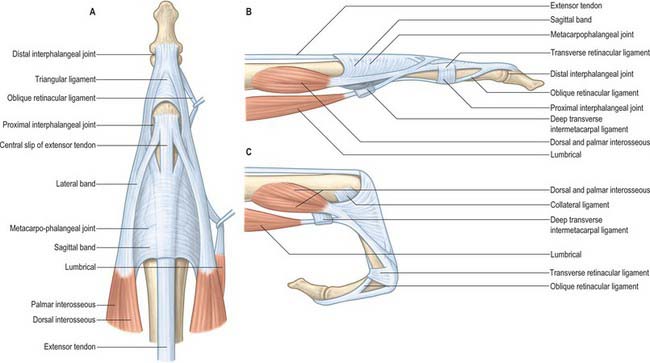
The superficial fascia within the finger is fibrofatty in the palmar and dorsal aspects, but more sheet-like laterally, where it is termed the lateral digital sheet. Within the core of the finger the fascia is thickened in areas, forming the flexor sheath, Cleland’s, Grayson’s and Landsmeer’s ligaments (Fig. 50.4). The flexor sheath is discussed in detail on page 879. Cleland’s ligaments extend from the sides of the phalanges, pass dorsal to the neurovascular bundles and insert into the lateral digital sheet. Grayson’s ligaments are more delicate, may even be discontinuous and pass from the lateral sides of the phalanges volar to the neurovascular bundles to insert into the lateral digital sheet. Landsmeer’s ligaments are inconsistent anatomical structures made up of transverse and oblique retinacular ligaments (see Fig. 50.30). The transverse retinacular ligament passes from the A3 pulley of the fibrous flexor sheath at the level of the proximal interphalangeal joint to the lateral border of the lateral extensor band. The oblique retinacular ligament lies deep to the transverse retinacular ligament. It originates from the lateral aspect of the proximal phalanx and flexor sheath (A2 pulley) and passes volar to the axis of rotation of the proximal interphalangeal joint in a dorsal and distal direction to insert into the terminal extensor tendon.
Functions of the fascia of the hand
Channelling of structures in transit between forearm and digits
The vertical septa act as spacers between the tendons and neurovascular bundles of the individual digital rays. Where tendons change direction around a concave surface the channels are thickened. They perform a retinacular role, forming sheaths with specialized pulleys to prevent the tendon springing away from the underlying skeleton (see flexor tendon sheaths, p. 879).
Digital and palmar spaces
There are many potential spaces within the hand, often with ill-defined margins.
The nail fold is a ‘U-shaped’ space made up of the eponychium and the lateral nail fold. The apical spaces at the tip of the finger are formed by the fibrous attachments of the distal phalanx to the tip of the digital pulp skin. The digital pulp spaces are confined compartments bounded by the digital creases which overlie the joints, and are attached to the underlying pulleys. The synovial flexor tendon sheaths are described on page 879. The web space is bounded distally by the skin and natatory ligament, by the deep transverse metacarpal ligament posteriorly, and by the deep attachments of the palmar fascia, together with their lateral attachments to the tendon sheaths proximally. The deep palmar space is a complex three-dimensional space limited proximally by the carpal tunnel. It lies deep to the palmar aponeurosis, between the radial and ulnar condensations of vertical fibres which connect the palmar aponeurosis to the thenar and hypothenar eminences. Partitions that pass deeply from the longitudinal bands of the palmar aponeurosis form eight narrow compartments: four contain the digital flexor tendons and four contain the lumbricals and the neurovascular bundles.
BONE
CARPAL BONES
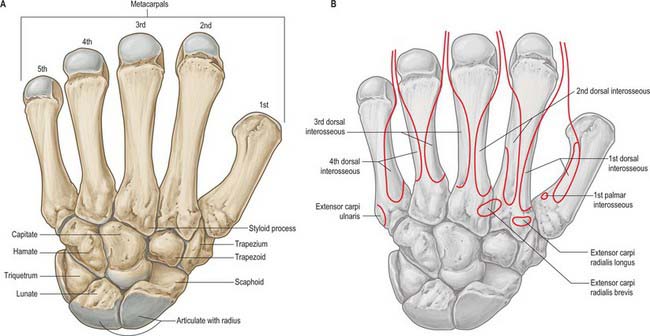
The carpus contains eight bones: four each in proximal and distal rows (Fig. 50.5 and Fig. 50.6). In radial (lateral) to ulnar (medial) order, the scaphoid, lunate, triquetrum and pisiform make up the proximal row, and the trapezium, trapezoid, capitate and hamate make up the distal row. The pisiform articulates with the palmar surface of the triquetrum, and is thus separated from the other carpal bones, all of which articulate with their neighbours. The other three proximal bones form an arch which is proximally convex, and which articulates with the radius and articular disc of the distal radio-ulnar joint. The concavity of the arch is a distal recess embracing, proximally, the projecting aspects of the capitate and hamate. The two rows of carpal bones are thus mutually and firmly adapted without any loss of movement.
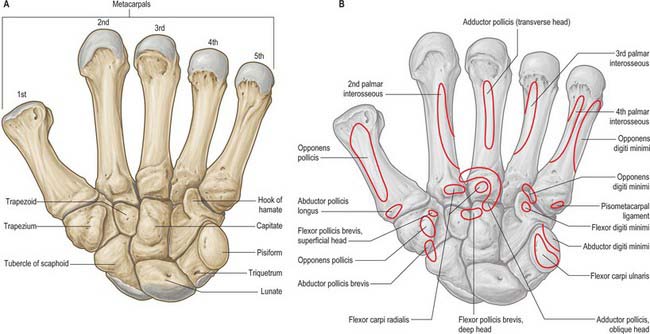
The dorsal carpal surface is convex. The palmar surface forms a deeply concave carpal groove, accentuated by the palmar projection of the radial (lateral) and ulnar (medial) borders. The ulnar projection is formed by the pisiform and the hamulus (hook), an unciform palmar process of the hamate. The pisiform is at the proximal border of the hypothenar eminence, on the ulnar side of the palm, and it is easily felt in front of the triquetrum. The hamulus is concave in a radial direction, its tip is palpable 2.5 cm distal to the pisiform, in line with the radial border of the ring finger. The superficial division of the ulnar nerve can be rolled on it. The radial border of the carpal groove is formed by the tubercles of the scaphoid and trapezium. The former is distal on the anterior scaphoid surface and palpable (sometimes also visible) as a small medial knob at the proximal border of the palmar thenar eminence, radial to the tendon of flexor carpi radialis. The tubercle of the trapezium is a vertically rounded ridge on the anterior surface of the bone, slightly hollow medially and just distal and radial to the scaphoid tubercle: it is difficult to palpate. (Both the scaphoid and trapezium may be grasped individually, and moved passively, by firm pressure between an opposed index finger and thumb applied to the palmar surface and ‘anatomical snuff-box’ simultaneously.) The carpal groove is made into an osseofibrous carpal tunnel by a fibrous retinaculum attached to its margins. The tunnel carries flexor tendons and the median nerve into the hand. The retinaculum strengthens the carpus and augments flexor efficiency. Radiocarpal, intercarpal and carpometacarpal ligaments are attached to the palmar and dorsal surfaces of all of the carpal bones, except the triquetrum and pisiform.
Individual carpal bones
Scaphoid
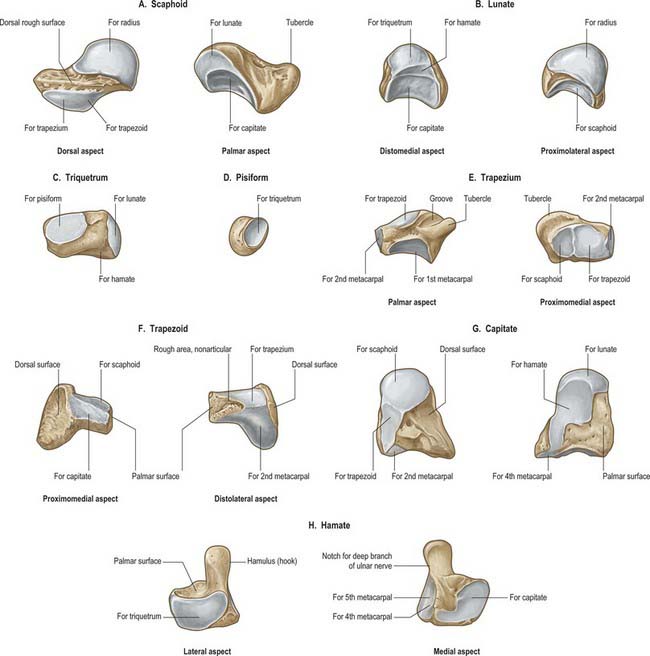
The scaphoid is the largest element in the proximal carpal row (Fig. 50.7A). It has a long axis which is distal, radial and slightly palmar in direction. A round tubercle on the distolateral part of its palmar surface is directed anterolaterally (Fig. 50.5), and provides an attachment for the flexor retinaculum and abductor pollicis brevis: it is crossed by the tendon of flexor carpi radialis. The rough dorsal surface is slightly grooved, narrower than the palmar, and pierced by small nutrient foramina, which are often restricted to the distal half (13%). The radial collateral ligament is attached to the lateral surface, which is also narrow and rough. The remaining surfaces are all articular. The radial (proximal) surface is convex, proximal and directed proximolaterally; the lunate surface is flat, semilunar, and faces medially; the capitate surface is large, concave and distal, and directed distomedially. The surface for the trapezium and trapezoid is continuous, convex and distal.
Lunate
The lunate is approximately semilunar and articulates between the scaphoid and triquetrum in the proximal carpal row (Fig. 50.7B). Its rough palmar surface, almost triangular, is larger and wider than the rough dorsal surface. Its smooth convex proximal surface articulates with the radius and the articular disc of the distal radio-ulnar joint. Its narrow lateral surface bears a flat semilunar facet for the scaphoid. The medial surface, almost square, articulates with the triquetrum and is separated from the distal surface by a curved ridge, usually somewhat concave for articulation with the edge of the hamate in adduction (Fig. 50.7B, left). The distal surface is deeply concave to fit the medial part of the head of the capitate.
Triquetrum
The triquetrum is somewhat pyramidal and bears an oval isolated facet for articulation with the pisiform on its distal palmar surface (Fig. 50.7C). Its medial and dorsal surfaces are confluent, and marked distally by the attachment of the ulnar collateral ligament, but smooth proximally to receive the articular disc of the distal radio-ulnar joint in full adduction. The hamate surface, lateral and distal, is concavoconvex, broad proximally, narrow distally. The lunate surface, almost square, is proximal and lateral.
Pisiform
The pisiform is shaped like a pea, with a distolateral long axis (Fig. 50.7D). It bears a dorsal flat articular facet for the triquetrum. The tendon of flexor carpi ulnaris and the distal continuations of the tendon, the pisometacarpal and pisohamate ligaments, are all attached to the palmar non-articular area, which surrounds and projects distal to the articular surface: the pisiform therefore has attributes of a sesamoid bone.
Trapezium
The trapezium has a tubercle and groove on its rough palmar surface (Fig. 50.7E). The groove, which is medial, contains the tendon of flexor carpi radialis, and two layers of the flexor retinaculum are attached to its margins. The tubercle is obscured by the thenar muscles which are attached to it (opponens pollicis, flexor pollicis brevis and abductor pollicis brevis) (Fig. 50.5B). The elongated, rough dorsal surface is related to the radial artery. The large lateral surface is rough for attachment of the radial collateral ligament and capsular ligament of the thumb carpometacarpal joint. A large sellar surface faces distolaterally and articulates with the base of the first metacarpal. Most distally it projects between the bases of the first and second metacarpal bones and carries a small, quadrilateral, distomedially directed facet which articulates with the base of the second metacarpal. The large medial surface is gently concave for articulation with the trapezoid. The proximal surface is a small, slightly concave facet for articulation with the scaphoid. Its ridge, or ‘summit’, fits the concavity of the first metacarpal base, and extends in a palmar and lateral direction, at an angle of approximately 60° with the plane of the second and third metacarpals. Abduction and adduction occur in the plane of the ridge, which is shorter than the corresponding metacarpal groove. Their contours vary reciprocally: they are more curved near the second metacarpal base, whereas the radius of curvature is longer further away from this site. The two surfaces are not completely congruent, and the area of close contact probably moves towards the palm in adduction and dorsally in abduction. While the axis of flexion/extension passes through the trapezium, that for adduction/abduction is in the metacarpal base. Flexion is accompanied by medial rotation, and extension by lateral rotation (p. 875).
Trapezoid
The trapezoid is small and irregular. It has a rough palmar surface which is narrower and smaller than its rough dorsal surface: the former invades the lateral aspect (Fig. 50.7F). The distal surface, which articulates with the grooved base of the second metacarpal, is triangular, convex transversely and concave at right angles to this. The medial surface articulates by a concave facet with the distal part of the capitate, the lateral surface articulates with the trapezium, and the proximal surface articulates with the scaphoid.
Capitate
The capitate is the central and largest carpal bone. It articulates with the base of the third metacarpal via its triangular distal concavoconvex surface (Fig. 50.7G). Its lateral border is a concave strip for articulation with the medial side of the base of the second metacarpal. Its dorsomedial angle usually bears a facet for articulation with the base of the fourth metacarpal. The head projects into the concavity formed by the lunate and scaphoid: the proximal surface articulates with the lunate, and the lateral surface with the scaphoid. The facets for the scaphoid and trapezoid, though usually continuous on the distolateral surface, may be separated by a rough interval. The medial surface bears a large facet for articulation with the hamate, which is deeper proximally where it is partly non-articular. Palmar and dorsal surfaces are roughened for carpal ligaments, the dorsal being the larger.
Hamate
The hamate is cuneiform and bears an unciform hamulus (hook) which projects from the distal part of its rough palmar surface. The hamulus is curved with a lateral concavity and its tip inclines laterally, contributing to the medial wall of the carpal tunnel (Fig. 50.7H). The flexor retinaculum is attached to the apex of the hamulus. Distally, on the hamular base, a slight transverse groove may be in contact with the terminal deep branch of the ulnar nerve. The remaining palmar surface, like the dorsal, is roughened for attachment of ligaments. A faint ridge divides the distal surface into a smaller lateral facet which articulates with the base of the fourth metacarpal base, and a medial facet for articulation with the base of the fifth. The proximal surface, the thin margin of the wedge, usually bears a narrow facet which contacts the lunate in adduction. The medial surface is a broad strip, convex proximally, concave distally, which articulates with the triquetrum: distally a narrow medial strip is non-articular. The lateral surface articulates with the capitate by a facet covering all but its distal palmar angle.
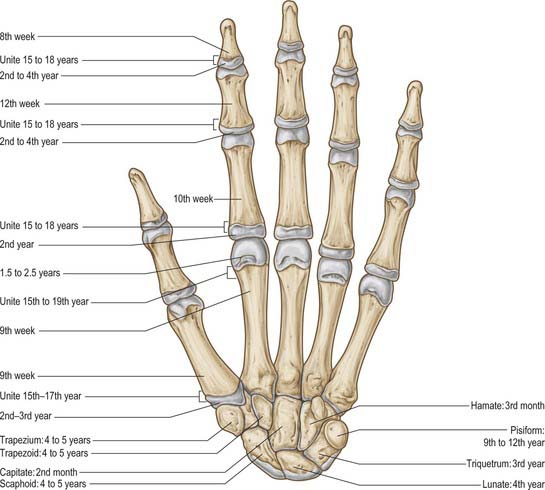
Ossification
Carpal bones are cartilaginous at birth, although ossification may have started in the capitate and hamate. Each carpal bone is ossified from one centre, capitate first, and pisiform last: the order in the others varies (Fig. 50.8, Fig. 5.9, Fig. 5.10, Fig. 5.11, Fig. 50.12). The capitate begins to ossify in the second month, the hamate at the end of the third month, the triquetrum in the third year, the lunate, scaphoid, trapezium and trapezoid in the fourth year in females and fifth year in males. The pisiform begins to ossify in the ninth or tenth year in females, and the twelfth in males. The order varies according to sex, nutrition and, possibly, race. Occasionally an os centrale occurs between the scaphoid, trapezoid and capitate bones: during the second prenatal month it is a cartilaginous nodule which usually fuses with the scaphoid. Occasionally, lunate and triquetral elements may fuse. Other fusions and accessory ossicles have also been described.

Fig. 50.8 Radiograph of a hand at 2½ years (male), dorsopalmar projection. Note early stages of ossification in the epiphyses at the proximal ends of the phalanges and first metacarpal; at the distal ends of the remaining metacarpals and radius; in the capitate, hamate and lunate. Typically, the centre for the lunate is preceded by the centre for the triquetrum. Compare with Figs 50.9 and 50.10.
METACARPALS
Individual metacarpal bones
First metacarpal
The first metacarpal is short and thick (Fig. 50.13A). Its dorsal (lateral) surface can be felt to face laterally; its long axis diverges distolaterally from its neighbour. The shaft is flattened, dorsally broad and transversely convex. The palmar (medial) surface is longitudinally concave and divided by a ridge into a larger lateral (anterior) and smaller medial (posterior) part. Opponens pollicis is attached to the radial border and adjoining palmar surface; the first dorsal interosseous muscle (radial head) is attached to its ulnar border and adjacent palmar surface. The base is concavoconvex and articulates with the trapezium. Abductor pollicis longus is attached on its lateral (palmar) side, the first palmar interosseous muscle to its ulnar side. The head is less convex than in other metacarpals and is transversely broad. Sesamoid bones glide on radial and ulnar articular eminences on its palmar aspect.
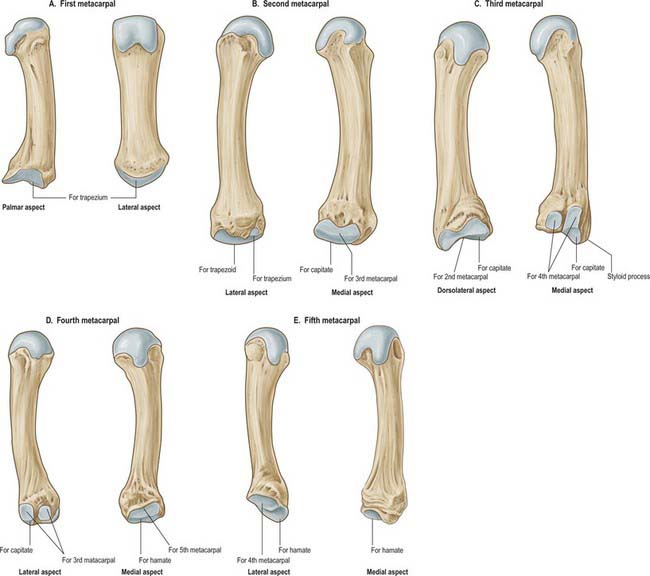
Second metacarpal
The second metacarpal has the longest shaft and largest base (Fig. 50.13B). The latter is grooved in a dorsopalmar direction for articulation with the trapezoid. Medial to the groove a deep ridge articulates with the capitate; laterally, nearer the dorsal surface of the base, there is a quadrilateral facet for articulation with the trapezium, and just dorsal to this facet a rough impression marks the attachment of extensor carpi radialis longus. On the palmar surface a small tubercle or ridge receives flexor carpi radialis. The medial side of the base articulates with that of the third metacarpal by a long facet, centrally narrowed. The shaft is prismatic in section and longitudinally curved, convex dorsally, concave towards the palm. Its dorsal surface is distally broad but proximally narrows to a ridge which is covered by extensor tendons of the index finger. Its converging borders begin at the tubercles, one on each side of its head for the attachment of collateral ligaments. Proximally the lateral surface inclines dorsally for the ulnar head of the first dorsal interosseous. The medial surface inclines similarly, and is divided by a faint ridge into a palmar strip for attachment of the second palmar interosseous, and a dorsal strip for attachment of the radial head of the second dorsal interosseous.
Third metacarpal
The third metacarpal has a short styloid process, projecting proximally from the radial side of the dorsal surface (Fig. 50.13C). Its base articulates with the capitate by a facet anteriorly convex but dorsally concave where it invades the styloid process on the lateral aspect of its base. A strip-like facet, constricted centrally, articulates with the bases of the second metacarpal (laterally) and the fourth metacarpal (medially), the latter by two oval facets. The palmar facet may be absent; less frequently the facets are connected proximally by a narrow bridge. The palmar surface of the base receives a slip from the tendon of flexor carpi radialis; extensor carpi radialis brevis is attached to its dorsal surface, beyond the styloid process. The shaft resembles that of the second metacarpal. The ulnar head of the second dorsal interosseous is attached to its lateral surface; the radial head of the third dorsal interosseous is attached to its medial surface, and the transverse head of adductor pollicis is attached to the intervening palmar ridge in its distal two-thirds. Its dorsal surface is covered by the extensor tendon.
Fourth metacarpal
The fourth metacarpal is shorter and thinner than the second and third (Fig. 50.13D). On its base it displays two lateral oval facets for articulation with the base of the third metacarpal; the dorsal is usually larger and proximally in contact with the capitate. A single medial elongated facet is for articulation with the base of the fifth metacarpal. The quadrangular proximal surface articulates with the hamate, and is anteriorly convex, dorsally concave. The shaft is like the second, but a faint ridge on its lateral surface separates the attachments of the third palmar interosseous and the ulnar head of the third dorsal interosseous. The radial head of the fourth dorsal interosseous is attached to the medial surface.
Fifth metacarpal
The fifth metacarpal (Fig. 50.13E) differs in its medial basal surface, which is non-articular and bears a tubercle for extensor carpi ulnaris. The lateral basal surface is a facet, transversely concave, convex from palm to dorsum, for articulation with the hamate. A lateral strip articulates with the base of the fourth metacarpal. The shaft bears a triangular dorsal area which almost reaches the base; the lateral surface inclines dorsally only at its proximal end. Opponens digiti minimi is attached to the medial surface. The lateral surface is divided by a ridge, which is sometimes sharp, into a palmar strip for the attachment of the fourth palmar interosseous and a dorsal strip for the ulnar part of the fourth dorsal interosseous.
Ossification
Each metacarpal ossifies from a primary centre for the shaft and a secondary centre which is in the base of the first metacarpal and in the heads of the other four (Figs 50.8–50.11). Ossification begins in the midshaft about the ninth week. Centres for the second to fifth metacarpal heads appear in that order in the second year in females, and between 1½ to 2½ years in males. They unite with the shafts about the 15th or 16th year in females, 18th or 19th in males. The first metacarpal base begins to ossify late in the second year in females, early in the third year in males, uniting before the 15th year in females and 17th in males. Sometimes the styloid process of the third metacarpal is a separate ossicle. The thumb metacarpal ossifies like a phalanx, and some authorities therefore consider that the thumb skeleton consists of three phalanges. Others believe that the distal phalanx represents fused middle and distal phalanges, a condition occasionally observed in the fifth toe. When the thumb has three phalanges, the metacarpal has a distal and a proximal epiphysis. It occasionally bifurcates distally. When it does, the medial branch has no distal epiphysis and bears two phalanges, while the lateral branch shows a distal epiphysis, and three phalanges. The existence of only a distal metacarpal epiphysis may be associated with a greater range of movement at the metacarpophalangeal joint. In the thumb, the carpometacarpal joint has the wider range, and the first metacarpal has a basal epiphysis. A distal epiphysis may appear in the first, and a proximal epiphysis in the second, metacarpal.

Fig. 50.9 Radiograph of a hand at 6½ years (male), dorsopalmar projection. Note the more advanced state of the centres of ossification which were already visible in Fig. 50.8, and the appearance of additional centres in the distal ulnar epiphysis and in the triquetrum, scaphoid, trapezium and trapezoid.

Fig. 50.10 Radiograph of a hand at 11 years (female), dorsopalmar projection. Note the maturing shapes of all the ossifications previously seen in Figs 50.8 and 50.9, with the addition of the pisiform.

PHALANGES
The phalanges of the little finger and the thumb differ. Abductor and flexor digiti minimi are attached to the medial side of the base of the proximal phalanx of the little finger. The tendon of extensor pollicis brevis and the oblique head of adductor pollicis (dorsally), and the oblique and transverse heads of adductor pollicis, sometimes conjoined with the first palmar interosseous (medially), are attached to the base of the proximal pollicial phalanx.
Ossification
Phalanges are ossified from a primary centre for the shaft and a proximal epiphysial centre (Figs 50.8–50.12). Ossification begins prenatally in shafts as follows: distal phalanges in the eighth or ninth week, proximal phalanges in the tenth, middle phalanges in the 11th week or later. Epiphysial centres appear in proximal phalanges early in the second year (females), and later in the same year (males), and in middle and distal phalanges in the second year (females), or third or fourth year (males). All epiphyses unite about the 15th to 16th year in females, and 17th to 18th year in males.
JOINTS
DISTAL RADIO-ULNAR JOINT
The distal radio-ulnar joint is a uniaxial pivot joint (Fig. 50.14).
RADIOCARPAL (WRIST) JOINT
The radiocarpal joint is a synovial biaxial and ellipsoid joint formed by articulation of the distal end of the radius and the triangular fibrocartilage with the scaphoid, lunate and triquetrum (Fig. 50.15 and Fig. 50.16). In the neutral position of the wrist, only the scaphoid and lunate are in contact with the radius and articular disc: the triquetrum comes into apposition with the disc only in full adduction of the wrist joint. The radial articular surface and distal discal surface form an almost elliptical, concave surface with a transverse long axis. The radial surface is bisected by a low ridge into two concavities. A similar ridge usually appears between the medial radial concavity and the concave distal discal surface. The proximal articular surfaces of the scaphoid, lunate and triquetrum, and their interosseous ligaments, form a smooth convex surface which is received into the proximal concavity.
CARPAL JOINTS
Wrist ligaments
Extrinsic ligaments
Extrinsic palmar carpal ligaments
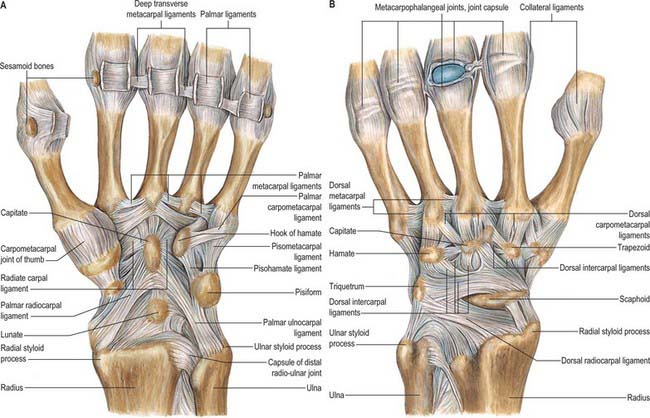
When the synovial lining of the carpal tunnel is dissected away, two V-shaped ligamentous bands are visible with their apices lying distally (Fig. 50.15A). The limbs of the ‘V’ take origin from the radius and ulna respectively: the apex of one ‘V’ attaches to the distal row and that of the second ‘V’ to the proximal row.
The long radiolunate ligament takes origin adjacent to the radioscaphocapitate ligament on the palmar lip of the radius. It passes over and supports the proximal pole of the scaphoid before inserting into the palmar horn of the lunate. This ligament is discrete from the radioscaphocapitate ligament and the visible separation is known as the interligamentous sulcus (continuous with the space of Poirier).
Extrinsic dorsal carpal ligaments
The dorsal wrist ligaments are comparatively thin. They are reinforced by the floor and septa of the fibrous tunnels for the six dorsal compartments. The extrinsic dorsal carpal ligaments and the intrinsic dorsal intercarpal ligaments have a ‘Z-shaped’ configuration (Fig. 50.15B). The pattern and shape of these ligaments is utilized in one surgical approach to the dorsum of the wrist joint where incisions are oriented parallel with the ligaments: this reduces scarring and restriction of subsequent motion caused by the arthrotomy.
Triangular fibrocartilage complex (TFCC) and distal radio-ulnar ligaments
The triangular fibrocartilage complex (TFCC) is a ligamentous and cartilaginous structure which suspends the distal radius and ulnar carpus from the distal ulna. The TFCC stabilizes the ulnocarpal and radio-ulnar joints, transmits and distributes load from the carpus to the ulna, and facilitates complex movements at the wrist (Fig. 50.17). By definition, it is made up of the cartilaginous disc, the meniscus homologue (an embryological remnant of the ‘ulnar’ wrist that is only occasionally present), volar and dorsal distal radio-ulnar ligaments, ulnar collateral ligament, floor of extensor carpi ulnaris subsheath, ulnolunate and ulnotriquetral ligaments. The triangular fibrocartilage proper (TFC) is a biconcave body composed of chondroid fibrocartilage. It extends across the dome of the ulnar head and varies between 2 and 5 mm in thickness.