The search for the causes of disease is an obvious central step in the pursuit of better health through disease prevention and Box 10.1, abstracted from a wonderful children’s picture book, illustrates perfectly the complexity of assigning causation. In the previous chapters we have looked at how we measure health (or disease) and how we look for associations between exposure and disease. Being able to identify a relation between a potential cause of disease and the disease itself is not enough, though. If our goal is to change practice or policy in order to improve health then we need to go one step further and decide whether the relation is causal because, if it is not, intervening will have no effect. As in previous chapters we will discuss causation mainly in the context of an exposure causing disease but, as you will see, when we come to assessing causation in practice, the concepts apply equally to a consideration of whether a potential preventive measure really does improve health.
As the story goes, there were five animals living by the sea, a cow, a donkey, a sheep, a pig and a mouse. One fine day they decided to go rowing on the bay.
First the cow got into the boat, it rocked a bit but she settled herself down comfortably at the back. Then the donkey got in carefully and sat down at the front to balance the boat. Next the pig climbed in, clutching her umbrella – the boat is low in the water by now. Then the sheep climbed in carrying her knitting and she sat down opposite the pig.
The boat is still afloat, but only just. Finally the little mouse jumped aboard and – disaster! The boat capsized and the animals had to swim to the shore.
So who sank the boat?
(Storyline (adapted) and pictures from Who Sank the Boat? by Pamela Allen, Copyright 1982. Published by Penguin Books Australia. Reproduced courtesy of Tim Curnow Literary Agent and Consultant, Sydney.)
What do we mean by a cause?
It is tempting to think that a cause is a single condition or event that inevitably leads to a particular effect or outcome; i.e. that there is a one-to-one relationship such that wherever or whenever the cause occurs the effect will follow. If we consider this more closely, it quickly becomes apparent that things are not so simple and that everyday causal phenomena are rather more complicated than they might seem at first. For example, while it might appear that all we need to do to turn on a computer is press the ‘on’ button, we know better: what if the wiring is faulty, there is no power supply or the hard drive has died an untimely death? To ‘cause’ the computer to come on we need power, good wiring, a functioning hard drive and relevant software in addition to the pressure of our finger on the button. We could describe each of these separate requirements as component causes, because they are all part of the one sufficient cause that will inevitably lead to the effect – in this case the computer turning on. In this situation they are also necessary causes because in the absence of just one of these things the computer will not work.
In the same way, disease rarely occurs as the result of a single event or exposure. Even though it might seem that an infectious agent would be a sufficient cause in its own right, not everyone develops disease following exposure to a particular bug. The real-life food-poisoning example in Chapter 1 made this clear – although people who ate the cold chicken were 3.8 times more likely to suffer from food poisoning than those who did not, almost one-quarter (23%) of those who ate the cold chicken suffered no ill effects. Whether someone does become ill depends both on their susceptibility to the agent and on the dose they receive. For tuberculosis (TB), for example, a person’s susceptibility is determined by whether they have been infected before and are now immune, and also their overall level of health at the time. The infectious agent, the tubercle bacillus, is only a component of the total or sufficient cause that will lead to TB. It is, however, a necessary cause in that, by definition, TB cannot occur without it. We will look at infectious diseases in more detail in Chapter 13.
Some definitions
There are many definitions of a cause, but the following, from Rothman (1986, p. 11), is appealing because of the brevity with which it captures the concept:
a cause is ‘an event, condition or characteristic [or a combination of these factors] that plays an essential role in producing an occurrence of the disease’
A more modern definition (Parascandola and Weed, 2001) that picks up on the concept of the ‘counterfactual’ that we discussed in Chapter 4 is that a cause is
something that makes a difference in the outcome (or the probability of the outcome) when it is present compared with when it is absent, while all else is held constant
The key to this second definition is that ‘all else is held constant’, something that is almost always impossible to achieve in real life. It also allows that a ‘cause’ may not always produce disease but may just increase (or reduce) the chance that disease will develop.
There are also many ways in which such entities (causes) can be classified, but the following subdivision serves well.
A sufficient cause is a factor (or more usually a combination of several factors) that will inevitably produce disease.
A component cause is a factor that contributes towards disease causation but is not sufficient to cause disease on its own.
A necessary cause is any agent (or component cause) that is required for the development of a given disease (for example, the specific infectious agent).
In terms of working out ‘who sank the boat’ we can say that each one of the animals was a component cause and that together they created the sufficient cause that caused the disaster. Probably none was actually necessary to sink the boat – any group of similarly sized animals would have had a similar effect. The ordering of the events, i.e. whether the mouse got in first or last, also did not matter; it was the sum of the weights that caused the boat to sink. This may also be true in much disease causation, but sometimes the component causes will have to occur in a specific order or they will have to be present at the same time. For example, TB infection will occur only if the individual is susceptible at the time they are exposed to the infection; and thrombosis (blood clotting) in an artery leading to a heart attack or stroke rarely occurs unless the blood vessel is already damaged or partly blocked.
A useful model for considering causal mechanisms is the ‘pie’ diagrams used by Rothman (1976) and shown in Figure 10.1. In this scheme:
I, II and III are three different sufficient causes for a disease;
A is a necessary cause for the disease because it is present in all three sufficient causes (assuming there are no other sufficient causes that do not include A); and
A, B, C, D, E, F, G, H, I and J are all component causes of one or other of the sufficient causes.
So, for example, if ‘A’ were the cow, ‘B’ the donkey, ‘C’ the pig, ‘D’ the sheep and ‘E’ the mouse, we would have sufficient cause I, while the other ‘pies’ show that different combinations of animals or other objects would also have led to the boat overturning.
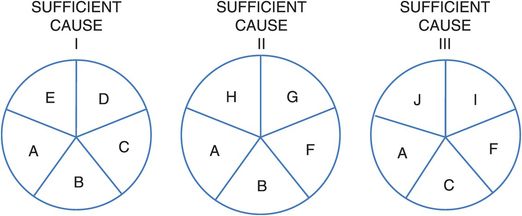
A conceptual scheme for the causes of a hypothetical disease.
In practice, when considering causes of disease we mostly find ourselves dealing with component causes. Aside from something like a major disaster such as an earthquake or nuclear explosion, it is hard to imagine identifying a single factor that is truly necessary and sufficient to cause disease. We also have to accept that, other than for something like an injury, we are unlikely to know either the precise nature of any sufficient cause or many of the possible component causes of disease. This need not matter – we do not have to eliminate all components of a particular cause in order to prevent disease due to that cause. If any one of them is identified and removed (e.g. B in the example above), then we will prevent cases of disease due to sufficient causes that contain component B (i.e. I and II). Some disease will still occur, however, as a result of sufficient cause III.
The causes of many diseases, and especially those like cancer that develop over many years, are going to be complex and we may never identify all their components. It is thus encouraging to know that by just identifying one or two we may still prevent a large proportion of the disease. If we could have stopped any one of the animals, even the mouse, from getting into the boat then it would not have turned over at that point in time. However, if the wind blew up or a wave came along once they had pushed off then they may have sunk later: a different sufficient cause leading to a similar outcome. Searching for modifiable causes that are associated with a large population attributable risk, i.e. those which cause a large number of cases of disease, will give the greatest benefit in terms of public health. (We will take this up again in Chapter 14.)
To be strictly accurate, we will only prevent the disease occurring at that point in time. In practice we may not prevent it completely, but might simply delay the onset. This is most obvious if we consider premature mortality; while we may be able to help someone live longer, e.g. by stopping them from smoking, we cannot prevent death completely.
Look at Table 10.1. The proportions of DALYs for cardiovascular and circulatory diseases attributable to the various risk factors sum to more than 100%. Why is this so? Is it a problem?
| Percentage of DALYs attributable to various risk factors | |||
|---|---|---|---|
| Developing | Developed | Global | |
| Dietary risks | 65 | 66 | 65 |
| High blood pressure | 56 | 58 | 57 |
| Tobacco smoking | 27 | 25 | 26 |
| Ambient particulate matter pollution | 21 | 11 | 18 |
| High body mass index | 13 | 29 | 17 |
| Physical inactivity | 15 | 20 | 16 |
| Household air pollution from solid fuels | 21 | 2 | 16 |
If we assume that each of the causes of cardiovascular and circulatory disease shown can be represented by one of the letters in Figure 10.1 (for example, if dietary risks were cause ‘A’, high blood pressure were cause ‘B’ and smoking were cause ‘C’), we can immediately see that the total amount of disease attributable to each component cause will be much greater than 100%. Ensuring that everyone had an adequate diet (i.e. removing cause ‘A’) would prevent all disease due to sufficient causes I, II and III. However, if we have already removed the problem of high blood pressure (cause ‘B’) and so prevented disease due to sufficient causes I and II, then the extra benefit of improving diet could only prevent the extra disease due to sufficient cause III. Similarly, although stopping everyone smoking would prevent some disease on its own, once we have removed the problems of diet and high blood pressure it would have little extra benefit.
In thinking about how component causes might act together, we need to keep in mind that in no sense need they be similar: one component might be the absence of a protective factor, and another the presence of a quite different harmful factor. For instance, if we consider the underlying causes of lung cancer we would probably find that cigarette smoke is a component in most sufficient causes. However, because not all smokers develop lung cancer we can surmise that smoking is not a sufficient cause on its own but also requires other factors (for example, weakened DNA-repair capacity) to complete a sufficient cause. Similarly, because lung cancer can develop in the absence of smoking, we can presume that there is at least one sufficient cause that does not have personal smoking as a component cause.
Association versus causation
In preceding chapters we have considered how we can determine whether a particular exposure is associated with the outcome of interest. The next stage is to determine whether such an association may be causal. Just because a particular exposure is associated with the development of a disease does not automatically imply cause and effect. We must attempt to draw appropriate causal inferences explicitly from our data, in the light of other evidence.
In London during the cholera epidemics of the nineteenth century one common belief, the ‘miasma’ theory, was that cholera was caused by noxious vapours in the air. While John Snow was conducting his pioneering work implicating contaminated water, William Farr, director of the Office of the Registrar General, was also interested in the transmission of cholera. He had noticed that cholera mortality seemed to be higher in lower-lying areas and so collected mortality data for a number of districts in London at different elevations. This revealed a dramatic inverse relation between elevation and mortality, and Farr was able to calculate a formula that could accurately predict the mortality rate for any given elevation. Figure 10.2 shows a graph of actual cholera death rates for various levels of elevation above the River Thames as well as the death rates predicted by Farr’s theory. These data were taken as strong evidence in favour of the miasma theory, under which it was felt that the vapours would be most concentrated and, therefore, most dangerous at lower elevations.
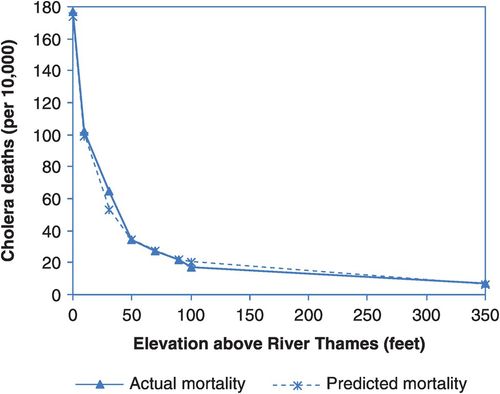
Actual (––) and predicted (- – – -) cholera death rates at various levels of elevation above the River Thames in London, England, 1849.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


