11 Water, electrolyte and acid-base balance
Salt and volume distribution
Water and volume
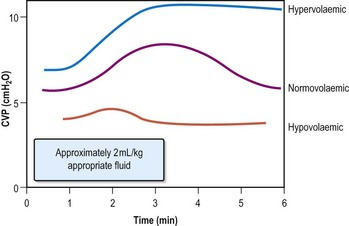
Assessing volume status
Thirst is a symptom of dehydration; oedema indicates increased volume.
Fluid therapy in hospital
Two common circumstances necessitate fluids as therapy (Table 11.1) in hospital:
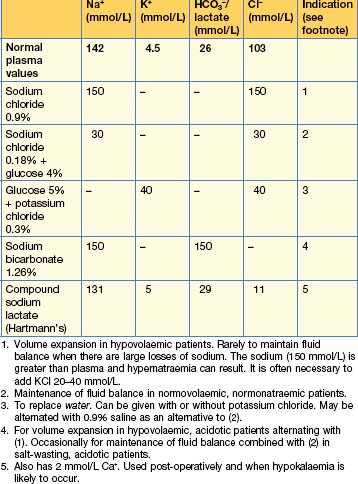
The volume administered varies according to the state of hydration; in otherwise well ‘nil by mouth’ patients with no losses, aim for 2 L/24 hours of saline (0.18%) and glucose (4%), usually with added potassium 20 mmol/L. Post-surgical fluid therapy should reflect the nature of the surgery (and the likely ongoing losses).
Sodium
Hyponatraemia
Investigations
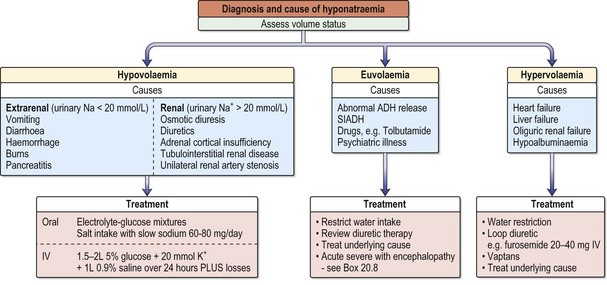
Hyponatraemia with a normal extracellular volume
Excess body water results from an abnormally high intake.
•Treating hyponatraemia without encephalopathy
•Treating hyponatraemia with encephalopathy, see Chapter 20, Emergencies in medicine, p. 711

Hyponatraemia with a decreased extracellular volume
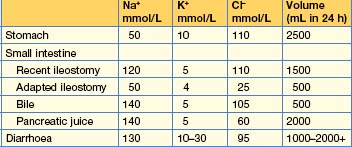
A decreased volume stimulates thirst and vasopressin release, which in turn inhibits water excretion. Losses from the kidney occur in tubulointerstitial disease, the recovery phase of acute tubular necrosis, unilateral renal artery stenosis, excessive use of diuretics, adrenocortical insufficiency and osmotic diuresis (e.g. hyperglycaemia, severe uraemia). Losses from the gastrointestinal tract are due to vomiting, diarrhoea, naso-gastric suction and haemorrhage (Table 11.2). Losses can also occur from the skin (burns), pericarditis and peritonitis.
Hyponatraemia with an increased extracellular volume



