Chapter 39 Vitamins, calcium, bone
Vitamins1 are substances that are essential for normal metabolism but are supplied chiefly in the diet.
Vitamins fall into two groups:
Vitamin A: retinol
Deficiency of retinol leads to xerophthalmia, squamous metaplasia, hyperkeratosis and impairment of the immune system.
Therapeutic uses
Retinol and derivatives provide therapeutic benefit in a number of clinical areas.
Psoriasis
Tazorotene, a topical retinoid, is effective in the treatment of chronic stable plaque psoriasis. Skin irritation is common, making it unsuitable for the treatment of inflammatory forms of psoriasis. The 0.05% cream is better tolerated than 0.1% although less effective. Acitretin is a retinoic acid derivative (t½ 48 h) that is used orally for severe psoriasis. Dose range 25 mg alternate days – 50 mg daily (see p. 262, as well as other disorders of keratinisation).
Acne
Tretinoin is retinoic acid and is used in acne by topical application (see p. 273). Isotretinoin is a retinoic acid isomer (t½ 20 h) given orally for acne (see p. 273). It is also effective for preventing second tumours in patients following treatment for primary squamous cell carcinoma of the head and neck.
Vitamin B complex
Niacin (nicotinic acid, B3)
is converted to nicotinamide, and subsequently to nicotinamide adenine dinucleotide (NAD) and nicotinamide adenine dinucleotide phosphate (NADPH), the cofactors that are essential for the oxidation–reduction reactions that comprise tissue respiration. Nicotinamide is used for nutritional purposes. Pellagra resulting from dietary deficiency of niacin is rarely seen in developed countries. Causes other than dietary include alcoholism, carcinoid syndrome and Hartnup disease. Nicotinic acid at pharmacological doses is used for the treatment of some hyperlipidaemias (see p. 444). Adverse effects include peripheral vasodilatation, unpleasant flushing, itching and fainting.
Vitamin D, calcium, parathyroid hormone, calcitonin, bisphosphonates, bone
Vitamin D
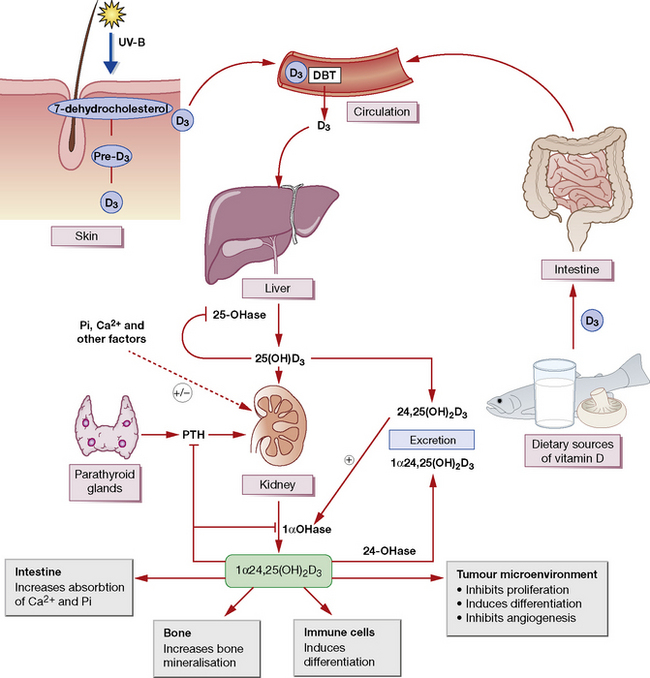
Vitamin D comprises a number of structurally related sterol compounds having similar biological properties (but different potencies) in that they prevent or cure the vitamin D-deficiency diseases, rickets and osteomalacia. The most relevant form of vitamin D is vitamin D3 (colecaciferol). This is made by ultraviolet irradiation of 7-dehydrocholesterol in the skin. It is also absorbed in the intestinal tract; however, few foods contain significant levels of vitamin D (Fig. 39.1). Vitamin D2 (ergocalciferol) is made by ultraviolet irradiation of ergosterol in plants. This is not the naturally occurring form.
Pharmacokinetics
Actions
are complex. Vitamin D promotes the active transport of calcium and phosphate in the gut (increased absorption) and renal tubule (reduced excretion), and thus controls, with PTH, the plasma calcium concentration and the mineralisation of bone (see Fig. 39.1). After a dose of D2 or D3 there is a lag of about 21 h before the intestinal effect begins; this is probably due to the time needed for its metabolic conversion to the more active forms. With the biologically more active calcitriol, the lag is only 2 h.



