Vesicating Agents Including Mustard and Lewisite
Stacey L. Hail
Daniel C. Keyes
MUSTARDS
Vesicating agents are chemicals named for causing blistering; they have a long military history. The mustards include mainly sulfur mustard and nitrogen mustard. Nitrogen mustard will not be discussed as it has not been stockpiled for military use and is largely used for chemotherapeutic purposes. Sulfur mustard (2,2-dichloroethyl sulfide) has been the most commonly used mustard compound.
Known also as mustard, mustard gas, “the king of war gases,” Yperite, H, and HD, sulfur mustard is one of the most powerful vesicants used as a chemical weapon (1,2). The chemical warfare agent H is an agent containing 70% sulfur mustard and 30% sulfur impurities. HD, however, is sulfur mustard purified by distillation and washing (3).
The term “mustard gas” is a misnomer because the agent is a liquid at typical environmental temperatures. Mustards are oily, yellow-brown, fat-soluble substances that are heavier than water. Mustard vapor has been described to smell like mustard, onion, garlic, or horseradish. Due to its low volatility, mustard concentrates in low-lying trenches and may persist in the environment for up to five days (3,4). At temperate climates with little wind, mustard may remain in the environment for more than a week. However, in areas with temperatures above 37.7°C, the agent may persist for only one day (2) (Table 2-1).
Sulfur mustard was discovered in 1822 by Belgian scientist Cesar-Mansuete Despretz (5), but was not used in battle until 1917 near Ypres, Belgium. That is how mustard earned the name Yperite. During World War I, mustard was responsible for as many as 400,000 battlefield injuries and 8,000 deaths (4). Interestingly, mustard accounted for 77% of World War I casualties (4). Thus, casualties from mustard gas were more numerous than those from any other agent used in World War I (6). Although several warring nations during World War II stockpiled sulfur mustard, there is little evidence that it was used in combat. In December 1943, an Allied ship carrying 100 tons of mustard was attacked by German planes and exploded near Bari, Italy. This attack caused mustard to disseminate over a large area producing mysterious ocular and dermal vesicant effects. This attack resulted in over 600 mustard casualties and numerous respiratory deaths (2,7). More recently, Iraqi forces during the Iran-Iraq conflict (1980 to 1988) used mustard causing as many as 3,000 Kurdish deaths (7). Iranian soldiers were evacuated to Europe where they were treated for classic mustard poisoning in the Iran-Iraq war (1,8). As recently as 1998, three American workers sustained mustard burns while collecting routine chemical samples from a storage site. All three individuals presented with blisters (9).
TABLE 2-1 Mustard Characteristics | |
|---|---|
|
THEORETICAL AND SCIENTIFIC BACKGROUND
Approximately 20% of sulfur mustard is rapidly absorbed through the skin (7,10). Due to the mustard’s fat solubility and its penetration down hair follicles and sweat glands, absorption occurs within 2 minutes. Twelve to 50% will react or remain “fixed” with skin components. The remainder will enter the systemic circulation and be absorbed by other tissues or solid organs. Once the sulfur mustard diffuses across a cell membrane, cell injury and cell death occurs. Although the exact mechanisms of sulfur mustard-induced cell death have yet to be elucidated, there are four proposed theories: (a) alkylation of deoxyribonucleic acid (DNA), (b) oxidative stress upon cell components, (c) depletion of glutathione, and (d) inflammatory responses (10).
Alkylation of DNA
An alkylating agent is an agent that replaces a proton on another molecule with an alkyl group (i.e., a simple chain of carbon atoms). DNA is cross-linked as a result of alkylation. The mustard alkylates the DNA, creating DNA strand breaks. This precipitates an increase in activity of various proteinases that may cause cellular damage and blister formation. DNA cross-linking also greatly inhibits further DNA synthesis. As DNA synthesis is inhibited, unbalanced growth of the cell occurs. Unbalanced cell growth triggers apoptosis, or programmed cell death (7,10).
Mustard changes the structure of DNA, cellular membranes and proteins through alkylation. After the mustard alkylates complementary strands of DNA, the molecules cannot separate. Separation of DNA molecules is needed for normal replication of DNA; therefore cell division is disturbed. Mustards exert their greatest effect on rapidly dividing cells (7).
Oxidative Stress
It is known that numerous biochemical reactions in the body and environmental sources generate highly reactive oxygen species (ROS) and free radicals that may cause cellular damage (11). Sulfur mustard is also believed to lead to oxidative stress upon intracellular molecules. As mustard diffuses across the cell membrane, it enters the aqueous environment of the cytosol. Within this aqueous media, sulfur mustard undergoes intramolecular cyclization creating a highly reactive episulfonium intermediate. This episulfonium ion reacts with functional groups on molecules, especially sulfhydryl-containing compounds. The episulfonium ion also reacts with the sulfhydryl groups on enzymes maintaining calcium homeostasis, thus leading to increased intracellular calcium. Increased cytosolic calcium leads to death in two ways. First, the calcium disrupts microfilaments that maintain cell integrity. The loss of cell integrity leads to cell death. Additionally, calcium induces apoptosis or programmed cell death (PCD) by activating endonucleases, proteases, and phospholipases (10).
Formation of this highly reactive episulfonium intermediate is greatly enhanced in an aqueous environment. Thus, moist regions such as mucosal tissues of the eye and respiratory tract are very susceptible to mustard injury (1).
Depletion Of Glutathione
Another theory of how mustard exposure causes injury is through depletion of glutathione. Reactive oxygen species (ROS) are normally detoxified by glutathione. However, in the setting of mustard, these ROS are left unchecked to react with membrane phospholipids forming lipid peroxidases. Lipid peroxidases cause loss of membrane function, membrane fluidity, and membrane integrity (10).
Inflammatory Response
After exposure to sulfur mustard, cells are stimulated to produce cytokines in response to the chemical stress. These cytokines are small peptides secreted by white blood cells and endothelial cells that cause immunologic reactions and further tissue damage (10).
SIGNS AND SYMPTOMS
Potentially, all organs can be affected by mustard exposure. However, the skin, eye, airway, bone marrow, gastrointestinal, and nervous system are particularly susceptible. One of the hallmarks of mustard intoxication is that it produces not only skin and eye effects but also systemic toxicity to internal organs such as the bone marrow. Clinical manifestations occur 2 to 48 hours after exposure, but typically are observed within 4 to 8 hours. The earlier signs and symptoms manifest, the more severe the exposure (4).
Skin
Skin is an important target for mustard since it contains frequently dividing cells. Eighty percent of mustard applied to human skin evaporates, with the remaining one-fifth of the agent penetrating and causing toxicity (7,10). Since sweat glands seem to facilitate mustard’s penetration through the skin, moist areas including the groin and axillae are particularly affected (12). In fact, scrotal and perianal burns were noted in nearly half of American survivors of World War I mustard gas attacks (2). Acute exposure is not associated with immediate discomfort or pain since the mustard has a long latency period (13).
Sulfur mustard produces cutaneous blisters and erythema in humans on areas directly exposed to the agent, often in areas covered by clothing. Burns may develop from exposure to the vapor or the liquid. The skin effects from vapor are dependent upon the ambient temperature and concentration. The concentration time (Ct) needed to produce erythema is 100 to 400 mg-min/m3, while onset of burns is about 200 to 1,000 mg-min/m3, and severe incapacitating burns result from 750 to 10,000 mg-min/m3. Erythema appears in affected areas within 2 to 4 hours and causes extreme pruritus. As the blisters appear, this itching diminishes. The blisters do not generally appear for 18 to 24 hours and contain large volumes of fluid. The fluid in the blister does not contain active mustard since the mustard completely reacts with the skin in the first several minutes (12).
Skin response to sulfur mustards has been described to have two phases: an immediate phase and a delayed phase. In the immediate phase, there is injury to the endothelium of superficial capillaries and venules due to direct damage to the cell membrane. Vascular leakage and infiltration with basophils may occur. The delayed phase is characterized by death of basal epidermal cells secondary to DNA damage, vascular leakage, neutrophilic immigration, and ulceration (7).
Human skin consists of two layers: a superficial layer, the epidermis, rests upon the dermis. The deepest layer of the epidermis is the stratum basale, which contains mitotically active keratinocytes. Between the epidermis and dermis is the basement membrane. This basement membrane is anchored to the keratinocytes in the epidermis by hemidesmosomes (Fig. 2-1). Sulfur mustard spares the basement membrane but disrupts the hemidesmosomes. Thus, a blister forms between the epidermis and the dermis leaving the basement membrane on the dermal side (12) (Fig. 2-2). Interestingly, there is racial variation in the severity of vesicant burns. Increased melanin appears to offer some protection (14).
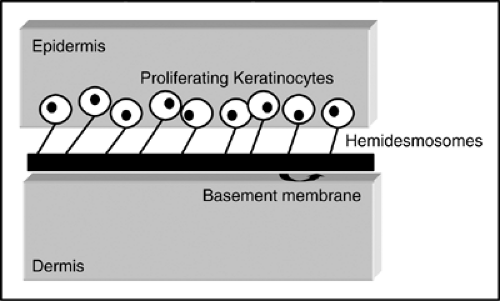 Figure 2-1. Schematic of normal skin. The basement membrane is located between the epidermis and the dermis. The proliferating keratinocytes are located at the base of the epidermis. They are anchored to the basement membrane by hemidesmosomes. |
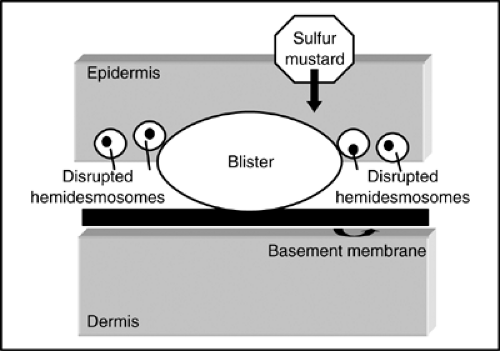 Figure 2-2. Schematic of skin after exposure to sulfur mustard. The sulfur mustard is rapidly absorbed. Injury occurs to the keratinocytes, and the hemidesmosomes are disrupted. Thus, a blister forms between the epidermis and the dermis. The basement membrane remains attached to the dermis. |
The burn caused by sulfur mustard behaves similarly to thermal burns in terms of depth, but it does not penetrate the skin as deeply as an acid burn. The skin effects can be classified as mild, moderate, or severe. Mild injuries involve erythema, edema, and first-degree burns and occur after exposure to doses of 50 mg-min/m3 or direct skin application 0.1 to 1.0 μg/cm2 liquid mustard. Moderate injury involves exposure to 1.0 to 2.5 mg/cm2 and leads to severe edema and vesication. Severe injury occurs after doses of 200 to 1,000 mg-min/m3 or direct skin application of more than 2.5 μg/cm2. At these doses, areas of necrosis are seen with surrounding vesication (2).
Mustard burns take twice the time to heal as thermal burns since the proliferating cells have been damaged (12). Experience with mustard gas casualties from the Iran-Iraq war demonstrated the slow resolution of these burns. Five soldiers with skin burns were managed with saline baths twice daily and dressings with silver sulfadiazine cream with paraffin gauze. Pain was severe and required opioids. None required skin grafting, but the healing process took 4 to 6 weeks (15). A characteristic brown pigmentation may be observed during the healing process and may even persist afterward (13).
Eye
In World War I and the Iran-Iraq war, 80% to 90% of casualties suffered ocular injuries. Injuries ranged from mild conjunctivitis to moderate and severe keratoconjunctivitis, which often lead to corneal damage. A World War I military physician documented: “12 hours after exposure, the patient’s eyes were inflamed and lacrimation, blepharospasm, and photophobia were present, … by the end of 24 hours the most distressing symptom was pain in the eyes, which was very severe. The patient was virtually blinded, with tears oozing from between the bulging, edematous eyelids, over his reddened blistered face” (16).
Mustard reacts rapidly after contact with eye tissues. In fact, mustard penetrates the cornea more rapidly than it does the skin (13). Symptoms, however, may be delayed for several hours (2,16). The aqueous-mucous surface of the cornea and conjunctiva facilitates absorption. Additionally, mustard solution is lipophilic so it concentrates in the oily moiety of the tears where it interacts with corneal epithelial cells. Because these corneal epithelial cells have a high turnover rate, they are some of the most vulnerable cells in the body. Initial symptoms include eye pain, photophobia, lacrimation, and blurred vision. Physical examination reveals blepharospasm (spasmodic winking), periorbital edema, conjunctival injection, and inflammation of the anterior chamber (9,16). For several days, the intraocular pressure may be elevated. Several hours later, the corneal epithelium begins to vesicate and slough. Visual acuity is decreased with worsening corneal injury. Ocular damage is classified as mild, moderate, or severe (2,16).
Mild injury occurs at doses of 12 to 70 mg/min/m3. At these doses, there is ocular irritation but little lacrimation, blepharospasm, or photophobia. On physical examination, there is mild erythema of the eyelids and conjunctiva. There is no corneal involvement. Complete recovery is often seen in several days (16).
Moderate ocular injuries are seen with doses of 100 to 200 mg/min/m3. Injury involves the eyelids, conjunctiva, and corneal epithelium with occasional iritis. Six hours after exposure, the patient complains of eye pain, eye dryness, photophobia, and possibly blindness. On examination, there is marked edema of the eyelids with blepharospasm. The conjunctiva is also edematous and congested. The cornea is edematous and fluorescein staining reveals punctate lesions at the palpebral fissure. There is gradual recovery after 48 hours. The corneal epithelium regenerates within 4 to 5 days. Complete symptomatic recovery takes at least 6 weeks (16).
Severe ocular injuries occur at doses higher than 200 mg/min/m3 and involve full-thickness corneal lesions. Symptoms include severe ocular pain, blepharospasm, and blurred vision. On physical examination, the eyelids are swollen, and there is conjunctival chemosis and loss of blood vessels at the nasal and temporal limbal areas. The cornea has been described to have an “orange peel appearance” and corneal sensation is weak or absent. Other findings in severe ocular injuries are pupillary constriction, iris vasodilatation, hemorrhages, and necrosis with development of chemical anterior uveitis leading to the formation of posterior iridolenticular synechiae, increased intraocular pressure, and opacification of
the lens. Resolution does not occur for 1 to 2 weeks. In 0.5% of casualties, delayed ulcerative keratitis leading to blindness may develop. These effects may be seen in patients up to 40 years after the mustard exposure (16).
the lens. Resolution does not occur for 1 to 2 weeks. In 0.5% of casualties, delayed ulcerative keratitis leading to blindness may develop. These effects may be seen in patients up to 40 years after the mustard exposure (16).
Battlefield mustard exposure results in the rapid visual incapacitation of large numbers of persons. During the Iran-Iraq conflict, 90% of individuals with mustard ocular injury were visually disabled for 10 days with conjunctivitis, photophobia, and minimal corneal swelling. The conjunctivitis and photosensitivity persisted in many patients for several months. Ninety percent of patients recovered completely from their ocular injuries (17).
Lungs and Airways
After eye lesions, the greatest acute discomfort produced by exposure to mustard is from injury to the respiratory system (13). Respiratory symptoms are also the most common cause of mortality (9). Pulmonary complications such as edema and airway obstruction are most responsible for deaths that occur soon after mustard exposure (4).
Low-dose inhalation of mustard gas causes chest tightness. Larger exposures result in sneezing, rhinorrhea, nasal bleeding, sore burning throat, hoarseness, and hacking cough. Cough may persist for 10 to 48 hours. Early signs of pulmonary edema, aphonia, and tachypnea may then occur. After 48 hours, bronchopneumonia appears (7). Fibrinous pseudomembranes can form, peel off, and lead to further airway obstruction (9,10).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


