Verrucous Squamous Cell Carcinoma
Lester D. R. Thompson, MD
Key Facts
Terminology
Highly differentiated, low-grade SCC variant characterized by exophytic growth with pushing borders and cytologically bland, amitotic squamous epithelium
Etiology/Pathogenesis
Strong association with tobacco and alcohol abuse, occasionally with HPV
Clinical Issues
Affects glottis, specifically anterior true vocal cords
Surgery alone seems to yield best outcome
˜ 20% recurrence/persistence rate overall (treatment dependent)
Pure VSCC does not metastasize
Macroscopic Features
Warty, exophytic, papillary or fungating tumor
Biopsy large enough to include deep margin and sufficient amount to make an accurate diagnosis
Microscopic Pathology
Multiple filiform, finger-like projections of well-differentiated squamous epithelium, maturing to surface
Abundant keratosis (ortho– and parakeratosis), “church spire” keratosis, with parakeratotic crypting
Broad pushing border of infiltration with dense inflammatory response
Top Differential Diagnoses
Verrucous hyperplasia, exophytic/papillary SCC, squamous papilloma, verruca vulgaris
 A low-power view shows a highly differentiated, exophytic, warty squamous neoplasm with pushing borders. There are papillary projections associated with extensive keratosis. This is an adequate biopsy. |
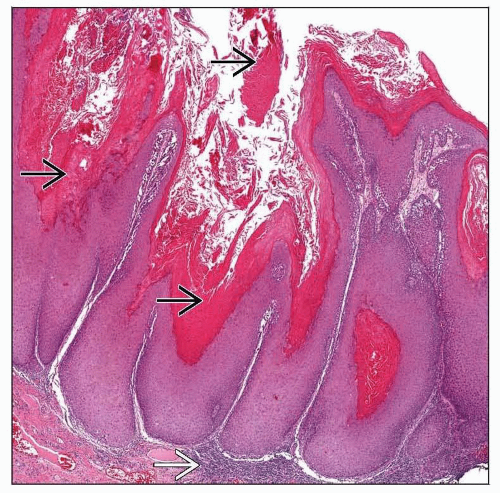 Broadly implanted, blunt-based, club-shaped papillae show maturation toward the surface. There is significant keratosis  , with a dense lymphoplasmacytic inflammatory basal response , with a dense lymphoplasmacytic inflammatory basal response  . . |
TERMINOLOGY
Abbreviations
Verrucous squamous cell carcinoma (VSCC)
Synonyms
Ackerman tumor
Verrucous acanthosis
Definitions
Highly differentiated, low-grade squamous cell carcinoma variant characterized by exophytic, warty neoplasm with pushing borders and cytologically bland, amitotic squamous epithelium
ETIOLOGY/PATHOGENESIS
Environmental Exposure
Strong association with tobacco and alcohol abuse
Infectious Agents
Human papillomavirus (HPV) genotypes 16 and 18 (rarely 6 and 11) are identified in some VSCC
CLINICAL ISSUES
Epidemiology
Incidence
Comprises up to 4% of all laryngeal SCC
Age
Mean: 6th and 7th decades
Gender
Male > Female (4:1)
In oral cavity, Female > Male (3:2)
Site
Larynx is 2nd most common site of VSCC
Oral cavity is most commonly affected (56%), then larynx (35%), sinonasal tract, and nasopharynx
Accounts for 15-35% of all VSCC
Glottis, specifically anterior true vocal cords
Supraglottis, subglottis, hypopharynx, and trachea uncommonly affected
Presentation
Long-lasting hoarseness is most common symptom
Other symptoms include airway obstruction, weight loss, dysphagia, and throat pain
Enlarged lymph nodes are common, but they are reactive rather than neoplastic
Endoscopic Findings
“Benign” papilloma-like appearance makes initial diagnosis difficult and may delay treatment
Broad-based, fungating, firm mass
May have extensive surrounding leukoplakia
Surface ulceration uncommon
Treatment
Options, risks, complications
Voice preservation strategies are encouraged
Even though neck lymph nodes appear enlarged, they are reactive, not representing metastatic disease
No neck dissection indicated
Surgery alone seems to yield best outcome
Radiotherapy
Theoretic risk of post-radiation anaplastic transformation
Rarely, post-radiation neoplasm may develop
Surgical approaches
Early (T1 or T2) tumors treated by local excision
Endoscopic resection (carbon dioxide [CO2] laser) or extended laser cordectomy
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


