FIGURE 26-1 Transtelephonic monitor (TTM) tracing demonstrating SVT. At first glance, the TTM demonstrates a wide QRS tachycardia. On further inspection, the QRS in sinus rhythm (*) is the same as the QRS in tachycardia (**). Patients with congenital heart disease commonly have a bundle branch block at baseline due to VSD repair. Therefore, it is important to determine not only the QRS duration but to determine whether the morphology is the same or different as that which is seen in sinus rhythm.
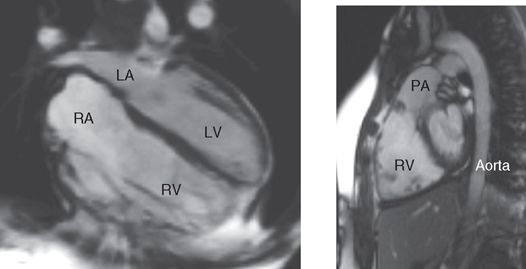
FIGURE 26-2 MRI of patient with TOF. This patient has a dilated RV and PA due to severe pulmonary regurgitation following TOF repair. Many patients require pulmonary valve replacement during late adolescence or early adulthood.
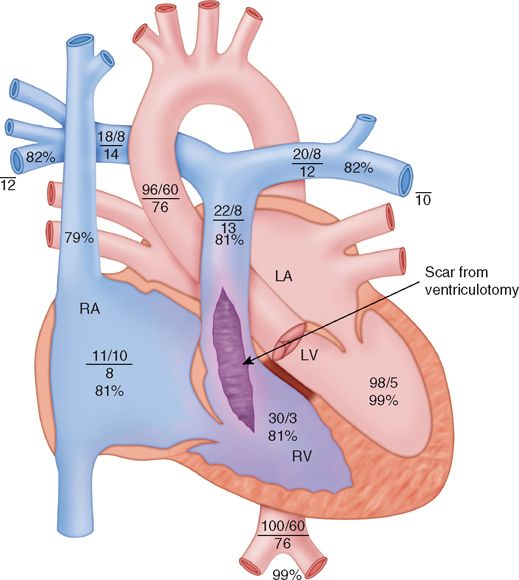
FIGURE 26-3 Cardiac catheterization diagram. The ventriculotomy incision was used to enlarge the RVOT, pulmonary valve, and MPA.
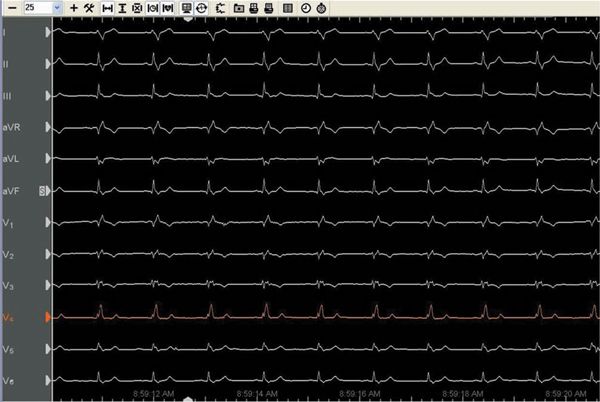
FIGURE 26-4 Baseline ECG. Note the wide QRS and the right bundle branch block which is classic in patients following TOF repair.
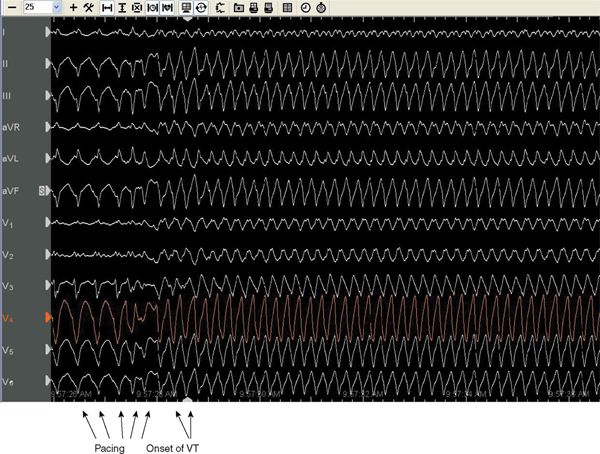
FIGURE 26-5 Surface electrograms of VT induction. Note the wide QRS and that it is different than the QRS in sinus rhythm.
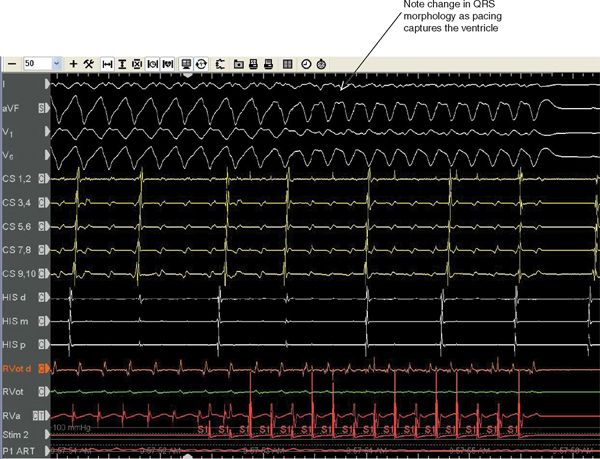
FIGURE 26-6 Burst pacing used to terminate VT. Note onset of pacing as seen as S1 on the Stim channel. Note the change in QRS morphology as pacing captures the ventricle.
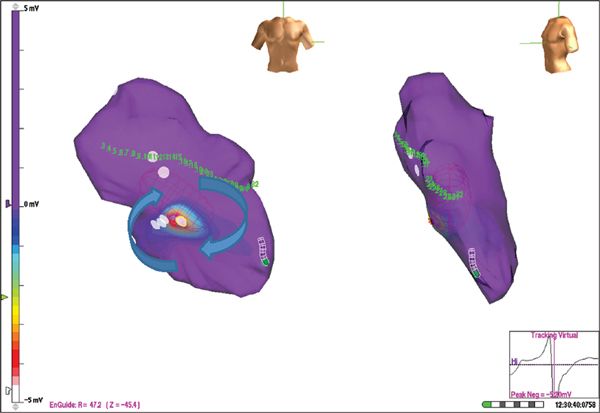
FIGURE 26-7 AP and lateral projections of right ventricle. In the image on the left, the white dots represent area of scar from ventriculotomy incision, and the blue arrows represent the circuit of the VT traveling between two areas of scar.
EPIDEMIOLOGY
• Congenital heart disease (CHD) is the most common form of birth defect with an incidence of 8 significant defects per 1000 live births.1 Due to advances in both diagnosis and treatment the majority of children live to adulthood. Over one million adult congenital heart disease patients are living in the United States.2 There are now a greater number of adults than children with congenital heart disease living in the United States.3
• Forty-five percent of these adults have simple defects (atrial septal defect, ventricular septal defect, valve stenosis).
• Forty percent have moderately complex heart disease (tetralogy of Fallot).
• Ventricular arrhythmias are rare among CHD patients during the first or second decade of life.
• Patients at highest risk for developing ventricular tachycardia are those who have undergone a ventriculotomy or patching of certain ventricular septal defects.
• Historically sudden cardiac death (SCD) in patients with CHD has been observed most often among patients with TOF and transposition of the great arteries (TGA) who are status post a Mustard or Senning operation4 (Figure 26-8).
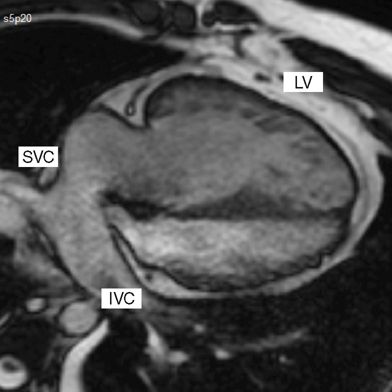
FIGURE 26-8 Transposition status post atrial baffle repair (Mustard or Senning repair). Note that the SVC and IVC blood is directed to the mitral valve and left ventricle, which is connected to the pulmonary artery. The pulmonary veins, not shown, are directed to the right ventricle, which is connected to the aorta.
• However, due to advances in surgical technique and timing of repair, a substantial shift in the epidemiology of mortality in CHD patients has occurred over the past 25 years. A comparison of mortality due to CHD between 1987 and 1988 and between 2004 and 2005 showed that the overall mortality rate had decreased by 31%.5 There has been a 40% reduction in annualized death rates for TOF and a 71% reduction for TGA between 1979 and 2005 in the United States.6 In patients with noncyanotic defects such as ventricular septal defects and coarctation of the aorta, arrhythmias were the leading cause of death before 1990, but after 1990 myocardial infarction was the leading cause of overall mortality. In those with cyanotic defects, ie, TOF and TGA, arrhythmias remain the leading cause of late death.
• Sustained VT appears to be the single biggest contributor to the 2% per decade incidence of sudden death in TOF.2
ETIOLOGY AND PATHOPHYSIOLOGY
• There are two main causes of ventricular arrhythmias in congenital heart disease. One is the result of the surgical scars from the repair, and the other is due to long-standing abnormal hemodynamics resulting from volume or pressure overload. Understanding the causes of the arrhythmia is only half the battle. One should understand that the surgical repairs have changed over time and the age at which these repairs are performed has also changed. This has contributed to the changing incidence of sudden cardiac death.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


