21 Vascular and endovascular surgery
Pathophysiology of arterial disease
Pathology
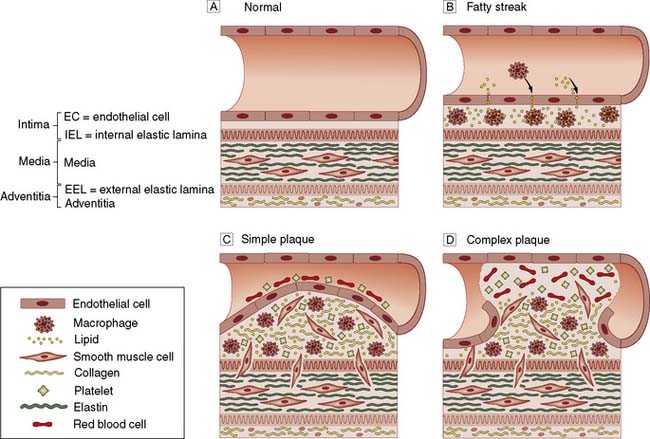
Most patients presenting to vascular specialists in developed countries have atherosclerosis which is characterized histopathologically by endothelial cell injury; sub-endothelial deposition of lipids and inflammatory cells; and smooth muscle cell migration and proliferation, all of which lead to plaque haemorrhage and rupture resulting in thrombosis and embolism (Fig. 21.1).
Clinical features
The clinical manifestations of arterial disease depend upon:
• Whether the artery is an end-artery or well collateralized
• The speed with which the disease develops
• Whether the underlying process is primarily haemodynamic, thrombotic, atheroembolic or thromboembolic, or due to aneurysmal dilatation or dissection
• The presence of other co-morbidity and the general condition of the patient.
Anatomical site
The patient’s symptoms and signs will depend upon the territory supplied by the affected artery:
• Coronary arteries: angina, myocardial infarction (MI)
• Cerebral circulation: stroke, transient ischaemic attack (TIA), amaurosis fugax, vertebrobasilar insufficiency (VBI)
• Renal arteries: hypertension, renal failure
• Mesenteric arteries: mesenteric angina, acute intestinal ischaemia
• Limbs: intermittent claudication (IC), chronic critical limb ischaemia (CLI), acute limb ischaemia.
Chronic lower limb arterial disease
Anatomy
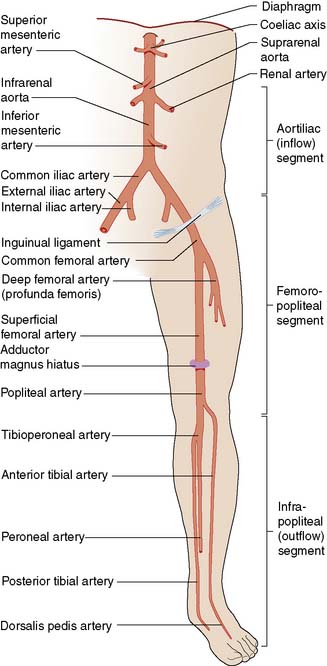
The lower limb arterial tree comprises the aortoiliac segment above the inguinal ligament (‘inflow’), the femoropopliteal segment and the infrapopliteal segment (‘outflow’) (Fig. 21.3).
Clinical features
Examination findings
On examination, the chronically ischaemic limb is usually characterized by:
• Pallor, particularly on elevation. Upon dependency, the foot becomes bright red; this is known as dependent rubor or ‘sunset foot’, and is due to reactive hyperaemia (Buerger’s test)
• Superficial veins that fill sluggishly in the horizontal position and empty upon minimal elevation (venous guttering)
• Nails that are brittle and crumbly
• Pulses that are weak or absent and sometimes associated with thrills on palpation and bruits on auscultation.

Intermittent claudication
Summary Box 21.1 Intermittent claudication (IC)
• IC is the most common manifestation of peripheral arterial disease, affecting up to 1 in 20 people over 60 years of age
• Limb loss is uncommon (up to 1–2% per year), but myocardial infarction and stroke are three times more common than in a non-claudicant population (up to 5–10% per year)
• The mainstays of treatment are risk factor modification (most importantly, complete and permanent smoking cessation), statin and antiplatelet (aspirin, clopidogrel) therapy and (supervised) exercise. This so-called Best Medical Therapy (BMT) leads to a clinically significant improvement in walking distance in the majority of patients; it also improves health related quality of life and increases longevity
• Patients should not normally be considered for surgical or endovascular intervention until they have been compliant with BMT for at least 6 months; intervention in the face of continued smoking is very unlikely to produce meaningful or durable benefit and is cost-ineffective
• Intervention includes angioplasty, stenting and bypass surgery. Long-term results are generally much better in the aorto-iliac segment than below the inguinal ligament.
Clinical features
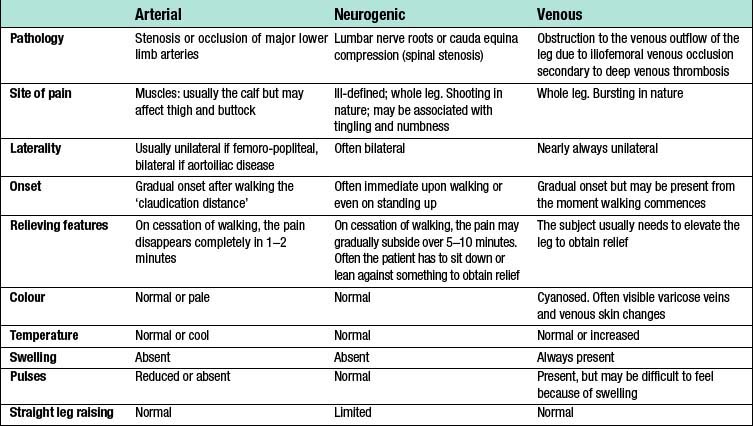
As lower limb arterial disease most frequently affects the SFA (Fig. 21.5), IC is usually characterized by pain on walking in the muscles of one or both calves. If the iliac arteries are affected then that pain may also be felt in the thigh and even the buttock (internal iliac disease). The pain comes on after a reasonably constant ‘claudication distance’, and usually subsides rapidly and completely on cessation of walking. Resumption of walking causes the pain to return. These and other features distinguish it from neurogenic and venous claudication (Table 21.1).

Fig. 21.5 Angiogram showing diffuse disease in both right and left superficial femoral arteries (arrows).
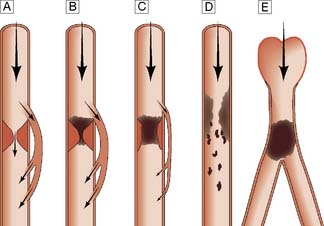
Typically, the superficial femoral artery (SFA) first becomes narrowed at the adductor canal (Fig. 21.6A). Ankle pulses may be palpable but are diminished, and a bruit may be heard at or below the stenosis. The ABPI is often (near) normal at rest but reduced following exercise.
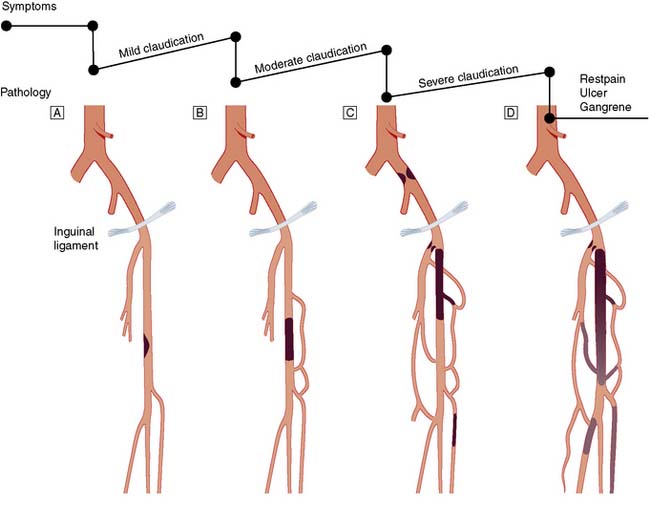
Over the next few months or years, collateral vessels arising from the PFA enlarge so that they carry a higher proportion of the blood flow to the lower leg. As a result, in the majority of patients, symptoms gradually improve or even disappear. But thrombotic occlusion of the SFA (Fig. 21.6B) may lead to a sudden deterioration in walking distance. Ankle and popliteal pulses will be absent at this stage.
Continued development of the collateral circulation may lead to an improvement in symptoms and walking distance. This phase of moderate claudication may remain apparently stable for several years. However, without ‘best medical therapy’ (BMT) (see below) and a change in the patient’s lifestyle, the atherosclerosis will progress to involve other segments, such as the PFA, iliac and tibial vessels (Fig. 21.6C). The IC will progress to become severe, often forcing the patient to stop every 50–100 metres or so, and the scope for spontaneous improvement steadily diminishes. As the disease progresses further in severity and extent, symptoms are likely to worsen to a point where CLI develops due to multilevel disease (Fig. 21.6D). Such patients will often go on to develop night/rest pain and are at risk of tissue loss (see below).
Critical limb ischaemia
Whereas IC is usually due to single-level disease, CLI (sometimes also termed severe limb ischaemia, SLI) is caused by multiple lesions affecting different arterial segments down the leg (Fig. 21.6D). These patients usually have tissue loss (ulceration or gangrene) and/or rest (night) pain; their ankle blood pressure is often 50–70 mmHg or less. Without revascularization, such patients will often lose their limb, and sometimes their life, in a matter of months.
Diabetic vascular disease
• Arteries are often calcified, which makes surgery and angioplasty technically difficult
• Calcification also leads to vessel incompressibility which results in spuriously high ankle pressures and ABPI measurements
• Reduced ability to fight infection
• Severe multisystem arterial disease (coronary, cerebral and peripheral), which increases the risks of intervention
• In the lower limbs, diabetic vascular disease has a predilection for the infrapopliteal vessels. Although vessels in the foot are often spared, the technical challenge of performing a satisfactory bypass or angioplasty to these small vessels is considerable
• Frequent coexisting neuropathy may lead to foot ulceration in its own right but may also complicate peripheral ischaemia (see below).
The diabetic foot
Motor neuropathy
The normal structure and function of the foot depends not only upon ligaments, but also upon the long and short flexors and extensors of the calf and foot. The former are affected more than the latter by motor neuropathy, leading to weakness and atrophy. The result is that the long extensors of the toes are unopposed and the toes become increasingly dorsiflexed. This exposes the metatarsal heads to abnormal pressure, and they are a frequent site of callus formation and ulceration (Fig. 21.7).

Management of lower limb ischaemia
Medical management
• Immediate, absolute and permanent cessation from smoking. This is by far the most important intervention and prognostic factor. In the face of continued smoking, other treatments are rendered largely ineffective and disease progression, limb loss and death (usually from cardiovascular causes) within a few years are the likely outcome.
• Control of hypertension according to current guidelines (for example, see the British Hypertension Society, www.bhsoc.org).
• Control of hypercholesterolaemia according to current guidelines (for example, see the British Heart Foundation, http://www.bhf.org.uk). All vascular patients should be prescribed lipid lowering drugs, usually a statin, so that their baseline total cholesterol is reduced by a third (ideally to below 4 mmol/l). Statins also stabilize atheromatous plaques and prevent the development and progression of aneurysmal disease through as yet incompletely understood anti-inflammatory mechanisms.
• Prescription of an antiplatelet agent (for guidance see National Institute of Clinical and Health Excellence, http://www.nice.org.uk/guidance/index.jsp?action=folder&o=51201). This is normally aspirin (75 mg daily) but clopidogrel (75 mg daily) is a more effective and safer alternative (but is also more expensive). Anticoagulation with warfarin should normally be reserved for patients with AF.
• Regular exercise as possible; it is widely accepted that supervised exercise in a health care environment is more effective than (unsupervised) simple advice to exercise.
• Control of obesity. This will help to bring down blood pressure, cholesterol and the ‘strain’ of walking; diabetes will also be easier to control. Surgical and endovascular intervention is much more difficult and morbid in obese patients.
• The identification and active treatment of patients with diabetes. This includes foot care (for further information see, for example, Diabetes UK, http://www.diabetes.co.uk).
Endovascular management
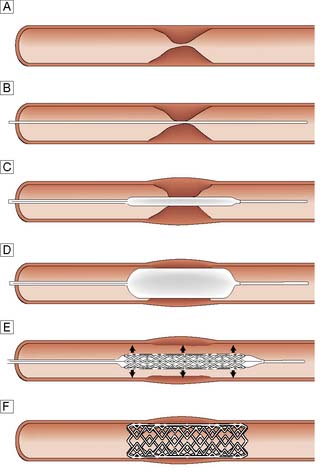
Balloon angioplasty (BAP), with or without stenting, has been used successfully in the iliac, femoral, popliteal and crural arteries and is usually performed under local anaesthesia (Fig. 21.8). The arterial lesion to be treated (stenosis or occlusion) is identified and crossed with a wire. A balloon catheter is introduced over the wire and the balloon inflated. This enlarges the lumen by disrupting the atheromatous plaque. In occlusions and complex disease, metal stents may be deployed across the lesion to improve patency and reduce distal embolic complications. Sometimes these balloons and stents are coated with drugs that reduce the arterial scarring (neo-intimal hyperplasia) that follows such intervention and can lead to restenosis and reocclusion (so-called drug eluting balloons and stents). Endoluminal repair of the aortoiliac segment is the treatment of choice in most vascular units because of its high patency rates, and low morbidity compared to open surgery. Infrainguinal BAP and, less commonly, stenting is also widely used in the management of IC and CLI.
Intermittent claudication
• tend to be younger, so that their symptoms have a greater impact on their quality of life and livelihood
• often have short-segment disease that is amenable to BAP, with or without a stent
• often have (relatively) normal infrainguinal arteries, so that restoring flow in the aortoiliac segment effects a dramatic improvement in the perfusion to their leg(s)
• tend to be more symptomatic, with shorter walking distances and bilateral symptoms
• may not achieve a satisfactory increase in walking distance with BMT alone, because the ability of the body to collateralize around aortoiliac disease is not as good as it is around femoropopliteal disease.
Critical limb ischaemia
The role of BAP and stenting in CLI remains controversial and, with present technology, many such patients remain unsuitable for endovascular therapy. The only published randomized controlled trial to compare BAP and bypass surgery (BSX) (http://basiltrial.com) indicates that although BAP is safer and less expensive than BSX in the short term (12–18 months), BSX (with vein) offers a more durable and complete revascularization in the longer term (3–5 years) (EBM 21.1). At the present time, CLI patients expected to only live 1–2 years and who do not have a suitable vein for the construction of a bypass are probably best treated by BAP where technically possible; all other CLI patients are probably best served by BSX. The role for endovascular therapy may increase in the future as technology improves.
Indications for arterial reconstruction
Intermittent claudication
Many surgeons are reluctant to perform infrainguinal bypass surgery for IC because:
• The risk of limb loss is very low with BMT
• Those patients who fail to comply with BMT (fail to stop smoking) are those most likely to press for surgery because of on-going symptoms. However, they are also those at greatest operative risk and those least likely to gain durable benefit from their bypass
• Surgery is associated with a significant risk of mortality and major morbidity, the size of that risk depending on the procedure and the patient but probably approaching 3–5% for infrainguinal bypass and 5–10% for aorto-bifemoral bypass
• As most patients have bilateral disease, even if they have unilateral symptoms, successful infrainguinal surgery on one side often reveals limiting IC symptoms on the other, requiring a second operation (the same for endoluminal treatment)
• Grafts have a finite patency, especially in those who fail to comply with BMT and, in particular, continue to smoke (the same for endoluminal treatment)
• As soon as a bypass graft is inserted, collaterals circumventing the original lesion shrink down. For this reason, when the graft occludes, usually suddenly, the patient is normally returned to a worse level of IC than before the operation. A patient who was previously a claudicant may now have acute limb-threatening ischaemia, which then forces the surgeon or radiologist to re-intervene. Secondary interventions are technically more difficult, are associated with higher risk and enjoy a lower patency rate.
Principles of arterial reconstruction
Endarterectomy
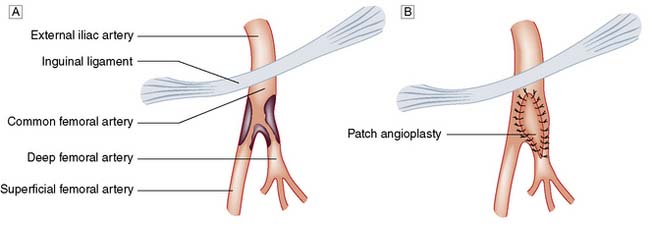
This involves the direct removal of atherosclerotic plaque and thrombus and is a relatively uncommon operation in modern vascular surgical practice except at the carotid and femoral bifurcations (Fig. 21.9).
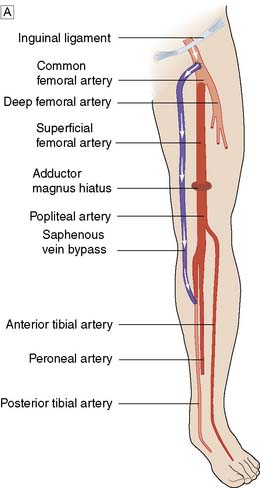
Bypass grafting
For a surgical bypass operation (Fig. 21.10) to be successful in the long term, three conditions must be fulfilled:
• There must be high-flow, high-pressure blood entering the graft (inflow)
• The conduit must be suitable
• The blood must have somewhere to go when it leaves the graft (outflow or run-off).

Two main types of conduit are available:
• autogenous material, most commonly the ipsilateral great saphenous vein (GSV)
• prosthetic material, most commonly expanded polytetrafluoroethylene (ePTFE) or Dacron.
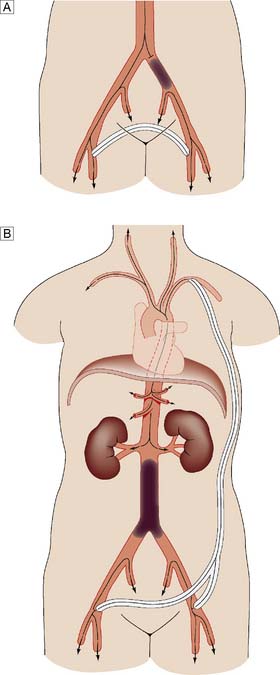
Extra-anatomic bypass
In most bypass operations, the new conduit more or less follows the course of the original artery – so-called anatomic bypass (Fig. 21.11). Where this is not possible and/or desirable, a so-called extra-anatomic bypass can be inserted (Fig. 21.12).
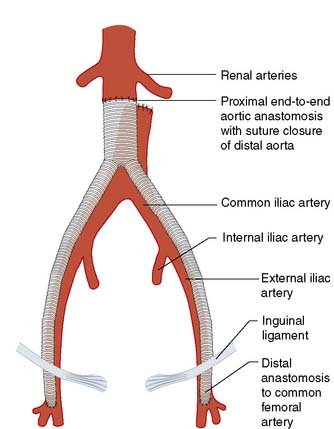
Fig. 21.11 Anatomic aortic bypass.
Reconstruction of an occluded aortoilliac segment by means of aorto-bi-femoral bypass grafting.
Amputation
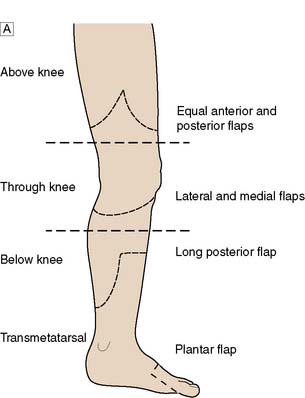
Level of amputation
This is determined by local blood supply, the status of the joints, the patient’s general health and his or her age. The broad principle is to amputate at the lowest level consistent with healing (Fig. 21.13). It is important to conserve the knee joint if at all possible, as the energy required to walk on a below-knee prosthesis is much less that required to walk on an above knee prosthesis. However, if the patient has other co-morbidity or disability that would make walking with a prosthesis impossible, there is no point in attempting to conserve the knee joint at the expense of healing. A common situation is where a patient presents with a fixed flexion contracture of the knee. A below-knee amputation in such a patient is usually ill-advised because the contracture will prevent the patient from ever walking and will also result in the stump wound resting on the bed or chair, leading to poor healing and wound breakdown.

Arterial disease of the upper limb
Overview
• Arm claudication. This is relatively unusual, even when the subclavian artery is completely occluded, because of collateral supply, mainly from the vertebral artery
• Atheroembolism to the hand. Small emboli lodge in the vessels of the fingers and the hand and lead to symptoms that are often mistaken for Raynaud’s phenomenon, except that in this case the symptoms are unilateral (see below)
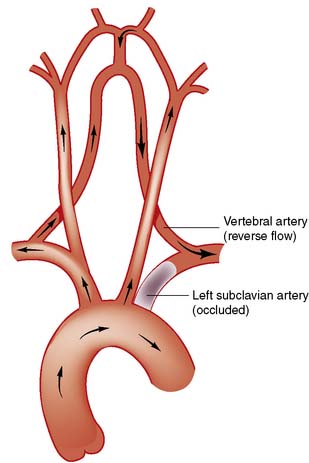
• Subclavian steal. In this circumstance, when the arm is used, blood is ‘stolen’ from the brain, with retrograde flow via the vertebral artery. This leads to vertebrobasilar ischaemia (VBI), characterized by dizziness, cortical blindness and/or collapse when the arm is used (Fig. 21.14).
Cerebrovascular disease
Carotid artery disease
Pathophysiology
Summary Box 21.2 Carotid artery disease
• Up to 50% of all ischaemic strokes may be caused by atheroembolism from the carotid bifurcation
• Patients with carotid territory transient ischaemic attacks (TIA) and amaurosis fugax should be assessed by a vascular surgeon with a view to carotid endarterectomy (CEA)
• When compared to BMT alone, CEA in addition to BMT significantly reduces the risk of further ipsilateral ischaemic stroke in patients with high grade symptomatic internal carotid artery stenosis
• CEA for asymptomatic internal carotid artery stenosis is controversial; such patients should be discussed with a vascular surgeon
• Several large trials have shown that with current technology, carotid artery stenting (CAS) can be an effective treatment for carotid stenoses, and should be considered as an option, particularly in patients at high risk for surgery.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


