23 Urological surgery
Assessment
Examination
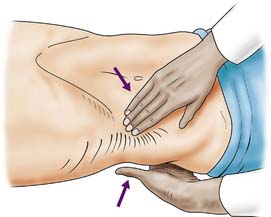
With the patient relaxed, the kidney can be balloted; lifted with one hand placed behind the loin and compressed by the other hand pressing downwards (Fig. 23.1). The ureter cannot be palpated. An enlarged bladder rises centrally out of the pelvis, is dull to percussion and may even be visible. In men, the hernial orifices, cords, testes and epididymes are examined with the patient standing and lying. If the foreskin is uncircumcised, it must be confirmed that it retracts and that the glans and meatus are normal. In women, the vulva, urethra and vagina must also be examined. A speculum examination should be carried out if there is any suspicion of vaginal or cervical abnormality. A full pelvic bimanual examination, whether in males or females, is best carried out under general anaesthesia with a muscle relaxant. A rectal examination is mandatory, not only to examine the prostate but also to detect abnormalities of the anal margin (haemorrhoids, fissures) and lower rectum (carcinoma).
Investigations
Intravenous urography (IVU)
A plain X-ray of the abdomen and pelvis is obtained to outline the areas of the kidneys, ureters and bladder (KUB film). The lumbar spine and pelvis, as well as stones in the region of the urinary tract, will be shown. An intravenous urogram (IVU) involves injecting iodine-containing contrast material intravenously and taking serial X-rays (Fig. 23.2) to demonstrate the renal pelvis and calyces, the rate of kidney emptying, the calibre of the ureters and the bladder outline. Once the bladder has filled, a ‘post-micturition’ film will demonstrate bladder emptying and the amount of residual urine.

Ultrasonography
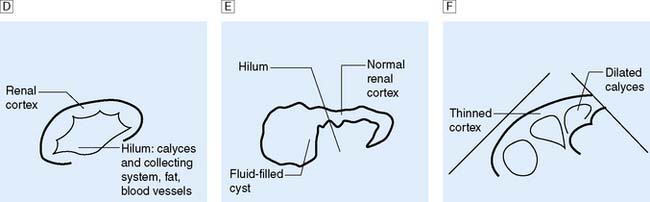
This is another means of first-line imaging (Fig. 23.3), tending to give superior information about the renal parenchyma but less about the collecting system. It also allows visualization of other related organs, such as the liver, spleen and gynaecological organs.



Special radiological investigations
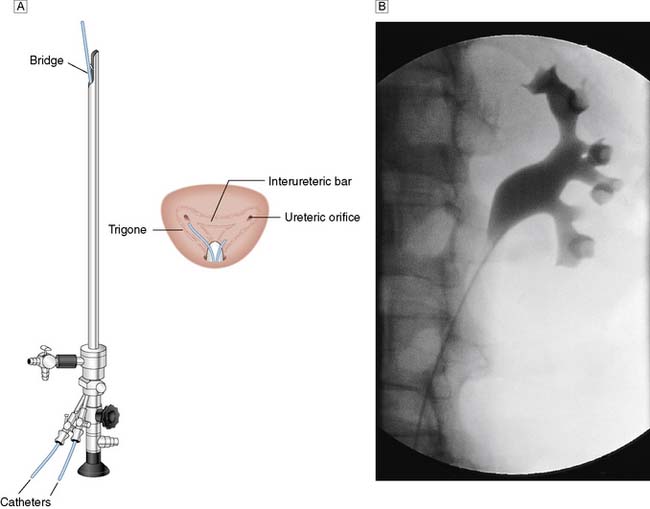
In certain circumstances a retrograde ureteropyelogram may be necessary. This involves retrograde injection of contrast material through a catheter placed in the lower ureter (Fig. 23.4). Abnormalities of the renal vessels can be demonstrated by renal angiography. Computed tomography (CT) is now the preferred method for imaging renal tumours. A micturating cystourethrogram (MCU) will outline the bladder, detect ureterovesical reflux and examine the bladder neck and urethra. The bladder is filled with contrast material (via a catheter) and emptying is then studied by X-ray screening. An ascending urethrogram, in which contrast medium is injected into the urethra, can be used to define strictures. When used in conjunction with a MCU, a descending urethrogram can also be obtained.
Nuclear imaging
Radio-labelled substances are used for two main purposes:
1. Detecting bony metastases from carcinoma of the prostate (bone scan). 99mTc-labelled methylene diphosphonate (MDP) is the most reliable method.
2. Measurement of renal function (scintigraphic renography). Occasionally ‘how a kidney looks’ does not correlate with ‘how it behaves’, e.g. hydronephrosis does not always mean the presence of obstruction. Renography allows assessment of obstruction to a kidney (e.g. from a pelviureteric obstruction), differential kidney function (i.e. how much each kidney is contributing to overall function), assess non-functioning areas of renal parenchyma (e.g. scarring) and allow accurate assessment of GFR. Radio-labelled mercaptuacetyltriglycine (MAG-3) has largely superseded technetium labeled diethylenetriamine pentaacetic acid (Tc-DTPA) for dynamic scanning. It is secreted from the renal tubules and is used in the identification of obstructed kidneys and to assess differential function. Dimercaptosuccinic acid (DMSA) is concentrated in the renal tubules and static imaging can be carried out some 2–3 hours after injection. Parenchymal defects such as scars, haematomas, lacerations or ischaemia may be demonstrated. Differential renal function can be quantified from measuring the DMSA concentration/density in each kidney.
Urodynamic studies
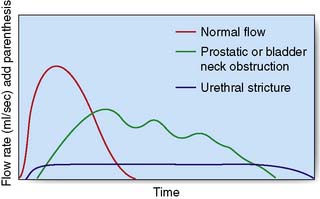
The maximum urinary flow rate during micturition can be measured using a flow meter when the voided volume is at least 150 ml or the values may be misleadingly low. The norm in males is 15–30 ml/s and in females 20–40 ml/s and a flow rate of less than 10 ml/s is abnormal. The flow rate pattern can help to determine the cause of obstruction (Fig. 23.5). Measurements of flow rate can be combined with cystometry to provide a measure of residual urine, bladder capacity, the capacity at which a desire to void occurs, and the detrusor pressures when the bladder is full and during maximum flow. Spontaneous detrusor contractions during bladder filling may indicate an unstable bladder, a cause of urgency and urge incontinence.
Upper urinary tract (kidney and ureter)
Anatomy
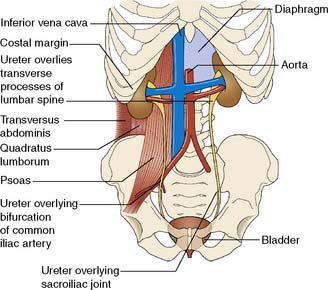
The two kidneys lie retroperitoneally on the posterior abdominal wall. Each is approximately 12 cm long, 6 cm wide and 3 cm thick. The upper pole of the kidney lies on the diaphragm, which separates it from the pleura and the 11th and 12th ribs. Below this, it lies on the psoas, quadratus lumborum and transversus abdominis muscles from medial to lateral (Fig. 23.6). Anteriorly, the right kidney is covered by the liver, the second part of the duodenum and the ascending colon. The spleen, stomach, tail of pancreas, left colon and small bowel overlie the left kidney. The renal hilum lies medially and transmits from front to back the renal vein, renal artery and renal pelvis. The ureter begins at the renal pelvis and runs for 25 cm to the bladder. The abdominal ureter lies on the medial edge of the psoas muscle, which separates it from the tips of the transverse processes. It then crosses the bifurcation of the common iliac artery, which separates it from the sacroiliac joint, to enter the pelvis. The pelvic ureter runs on the lateral pelvic wall to just in front of the ischial spine, when it then turns medially and forward to enter the bladder. In the male, it is crossed by the vas deferens. In the female, it lies close to the lateral fornix of the vagina and is crossed by the uterine vessels, where it is vulnerable to damage during hysterectomy. The section of ureter that lies within the bladder wall functions as a flap valve to prevent reflux. Stones tend to impact at the three points where the ureter narrows: namely, the pelviureteric junction, the pelvic brim and the ureteric orifice.
Renal adenocarcinoma
Investigations
The initial investigation is ultrasound, followed by a staging contrast CT of the abdomen and chest (Fig. 23.7).

Management
Summary Box 23.1 Renal carcinoma
• Renal adenocarcinoma is the most common malignant renal tumour and is twice as common in males
• The carcinoma arises in the renal tubules and spreads early to the renal pelvis, producing haematuria. Later spread involves the renal vein (with bloodstream dissemination), perinephric invasion and lymphatic spread
• The clinical presentation is very varied. The triad of pain, haematuria and a mass may be late features, and early systemic effects include fever, polycythaemia, disordered coagulation and pyrexia of unknown origin
• The key investigations are ultrasonography, chest X-ray and contrast CT
• Treatment consists of radical nephrectomy; the tumour is not radiosensitive. The natural history of renal carcinoma is very variable and excision of solitary metastases may be worthwhile.
Renal and ureteric calculi
Investigations
IVU or CT KUB provides all the necessary information on the position of the stone (Fig. 23.8). Routine hematological and biochemical tests are needed to assess renal function and to exclude metabolic causes. A urine sample is cultured to determine whether there is infection. If obstruction is acute, its relief is the prime clinical need; if it is chronic and has caused renal damage, the surgical approach depends on the function of the affected kidney. This is best determined by radioisotope methods (renography).


Upper tract obstruction
Obstruction may be due to extrinsic, intrinsic or intraluminal causes (Table 23.1). In the kidney, stones within the pelvicalyceal system and a congenital abnormality of the pelviureteric junction (see below) are the main causes of obstruction leading to hydronephrosis. More rarely, a sloughed renal papilla, blood clot or tumour may be the cause.
Table 23.1 Causes of urinary tract obstruction
| Extrinsic |
| Intrinsic |
| Intraluminal |
Pelviureteric junction obstruction (idiopathic hydronephrosis)
Management
Either laparoscopic or open pyeloplasty is performed to remove the obstructing tissue and refashion the pelviureteric junction (PUJ) so that the lower part of the renal pelvis drains freely into the ureter (Fig. 23.9). It is not possible to predict the degree of recovery of renal function after the relief of obstruction, but a kidney contributing less than 10% of total renal function should be removed.

Retroperitoneal fibrosis
Pathology
• Idiopathic. The aetiology is unknown, although it may be associated with methysergide or analgesic abuse Mediastinal fibrosis and Dupuytren’s contracture may coexist
• Malignant infiltration. The fibrosis contains malignant cells that have metastasized from primary sites such as the breast, stomach, pancreas and colon
• Reactive fibrosis. Radiotherapy, resolving blood clot, or extravasation of sclerosants can lead to fibrotic change in the retroperitoneum.
Management
Summary Box 23.2 Urinary tract obstruction
Common causes of obstruction of the lower outflow tract
• Benign prostatic hyperplasia
• Bladder cancer involving the bladder neck
• Bladder-neck obstruction (dyssynergia, infection, neurological disorders)
• Urethral obstruction (congenital posterior urethral valves, blocked urinary catheter, trauma, infection, stricture).
Common causes of obstruction of the upper urinary tract
• Renal and ureteric calculi (80% are calcium oxalate/phosphate stones)
• Pelviureteric junction obstruction (idiopathic hydronephrosis)
• Retroperitoneal fibrosis (idiopathic/malignant infiltration/radiotherapy)
• Transitional cell carcinoma (with or without bleeding and clot)
• Congenital abnormalities (e.g. ectopic ureter, ureterocoele)
Lower urinary tract (bladder, prostate and urethra)
Anatomy
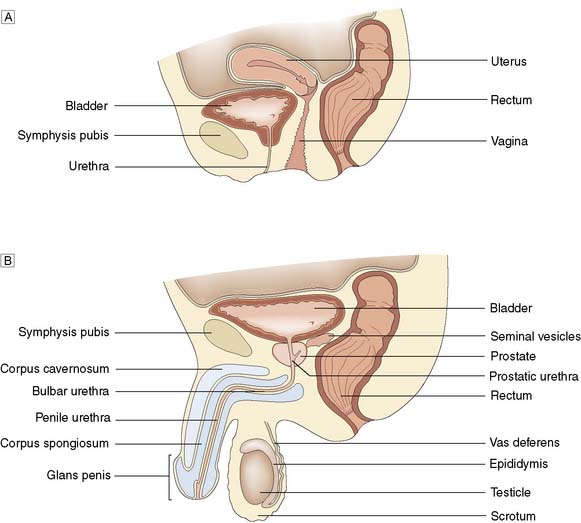
In the male, the prostate is pyramidal, with its base uppermost. It resembles the size and shape of a chestnut and surrounds the prostatic urethra. Traditionally described as having a median and two lateral lobes, it is better considered as being composed of a small central and a larger peripheral zone (Fig. 23.10).
Physiology
Trauma
Bladder
Closed injuries
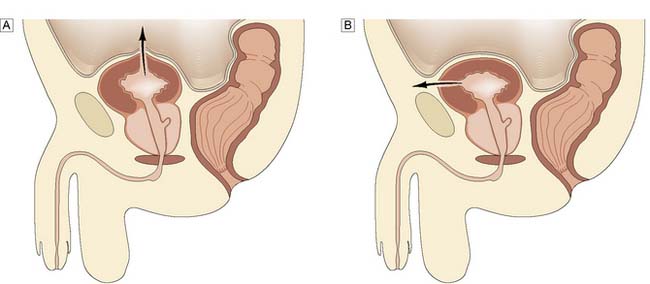
Intraperitoneal rupture typically occurs in a patient who has been drinking alcohol, has a full bladder and is assaulted and kicked in the abdomen. The dome of the bladder ruptures and urine extravasates into the peritoneum, causing intestinal ileus and abdominal distension. Extraperitoneal rupture is usually due to a major road traffic accident in which the pelvis has also been fractured when the bladder is not full, but may follow endoscopic resection of the prostate or a bladder tumour (Fig. 23.11).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


